
Dear students, before starting today’s lesson, I apologize for the poor quality of a few photos. During the first several seasons, Starz allow screen shots but this was stopped a while back. If I cannot find a needed image online, I take a photo of my TV screen. The results are often iffy. 🙄
That said, on with the lesson!
In Outlander episode 804, Muskets, Liberty and Sauerkraut, a strong wind announces an impending storm up so Claire closes a window and spies….

Guess who? None other than Elspeth Cunningham, aka, “wicked witch of the west” heading up the lane! 😜
Or, as Herself writes in “Go Tell the Bees that I am Gone” (Chapter 63, “The Third Floor”):
“As I leaned out with the shutter hook in my hand, though, I saw a tall black figure hastening toward the house, skirts and cloak flying in the wind.
“You and your little dog, too,” I murmured, and risked a glance at the forest, in case of flying monkeys.” 🐒
Mrs. Cunningham bursts through the door and lurches into Claire’s arms’ “I need your help.”

Yep! Elspeth does need Claire’s help! She fell against a settle and hurt her arm. (Pssst… A settle, if you don’t know, is a hardwood bench with arms and a high back) 😉
Wow! Claire knows what is wrong and claims she can fix it even before she examines the shoulder! 😳
This is pretty darn amazing, btw, because most physicians examine the injury first before stating they can fix whatever ails the patient. But, as Jamie says, “Claire, ye are a brilliant healer!”

Claire expose Elspeth’s injured right shoulder.
The nicely rounded contour of a normal shoulder is not what we see. Instead, Elspeth’s entire shoulder is angular and bony.
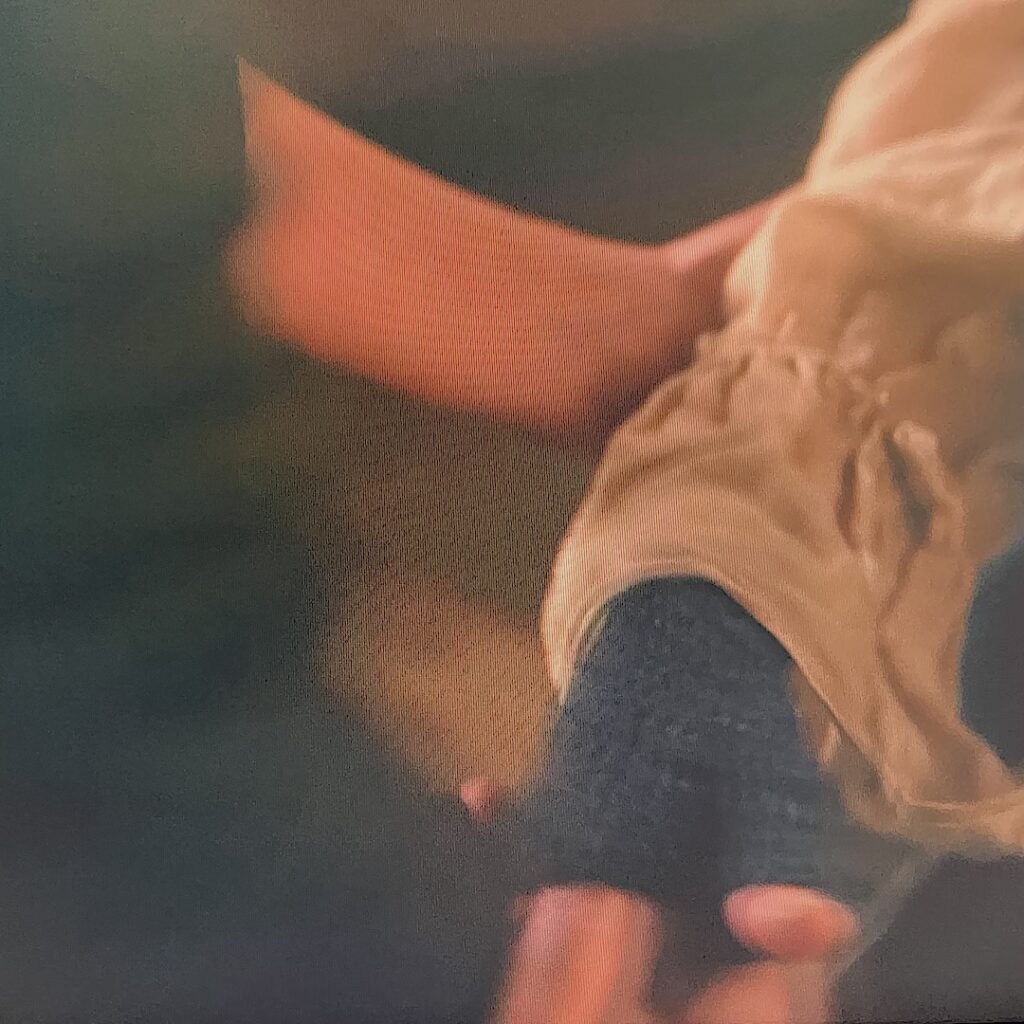
Claire tells Frances to give her some whisky and to “hold her,”

Claire warns Elspeth, it is gonna hurt. She grips the elbow and wrist and performs a quick maneuver. (Psst… more about this below)
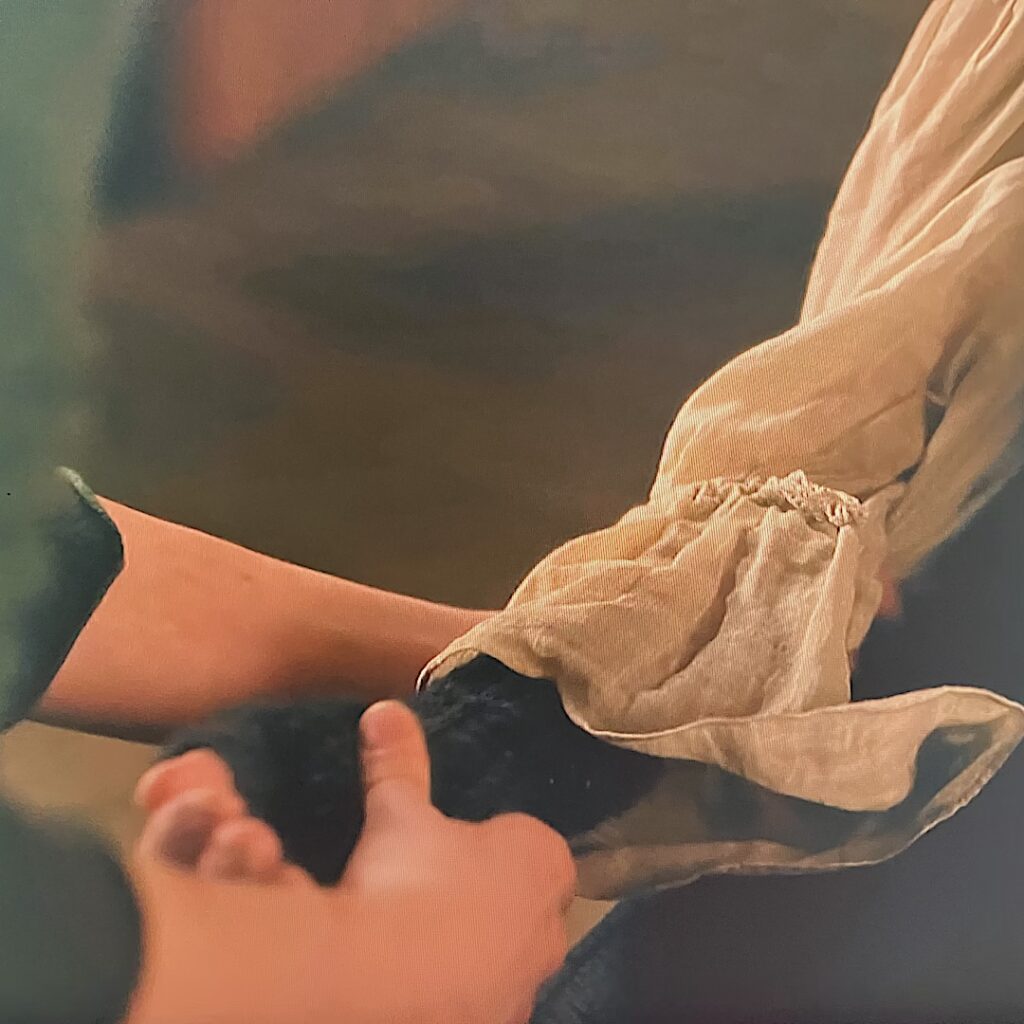
… and , voila! The shoulder pops back into joint.
“Grass-combing son of a buggering sod!” Elspeth exclaims!

Here, an excerpt from “Bees,” Chap. 63, “The Third Floor:”
“It’s been a long time since I heard language like that,” Fanny said, her lips twitching.
If you have to do with sailors, young woman, you acquire both their virtues and their vices.” Elspeth’s face was still white and shone like polished bone under a layer of sweat, but her voice was steady and her breath was coming back. “And where, might I ask, did you her language like that?”
Fanny glanced at me, but I nodded and she said simply, I loved in a brothel for some time, ma’am.”
“Indeed.” Mrs. Cunningham drew her wrist out of my grasp and sat up, rather shaky, but bracing herself with her good hand on the table. “I suppose whores must also have both virtues and vices, then.”
“I don’t know about the virtues,” Fanny said dubiously. “Unless you count being able to milk a man in two minutes by the clock.”
I had taken a nip of the whisky myself, and choked on it.
“I think that would be classed as a skill rather than a virtue.” Mrs. Cunningham told Fanny. “Though a valuable one, I daresay.”
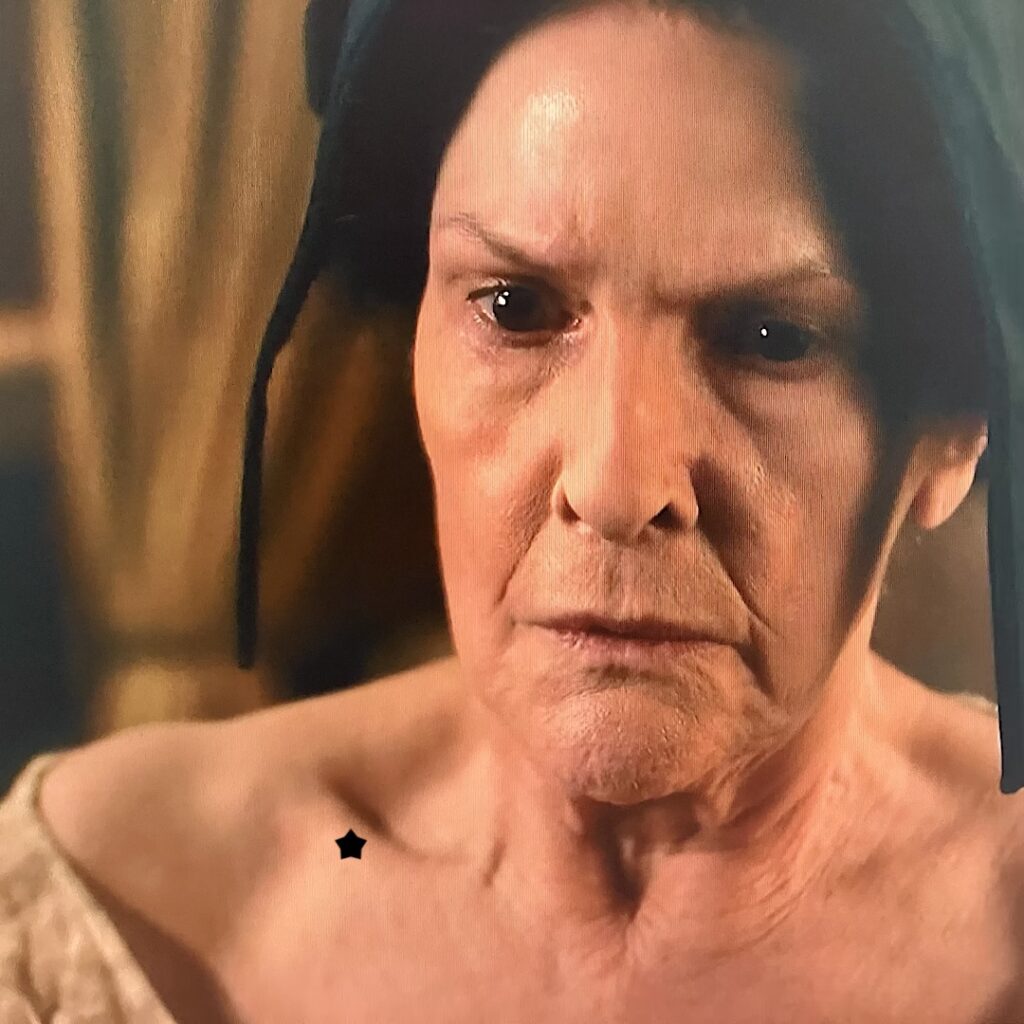
Mrs. Cunningham’s has a rather handsome shoulder, now. The rounded contour of the shoulder and function of her extremity is fully restored. Of course, it is going to be sore for a wee bit.
Note: I must say, the FX or prosthesis of the dislocation wasn’t too bad. My major criticism is the clavicle is too straight and long. It is a curved bone that stops short of the shoulder point as is evident in the next image (black star) post reduction.
Now for the anatomy lesson. Yay! 🤓
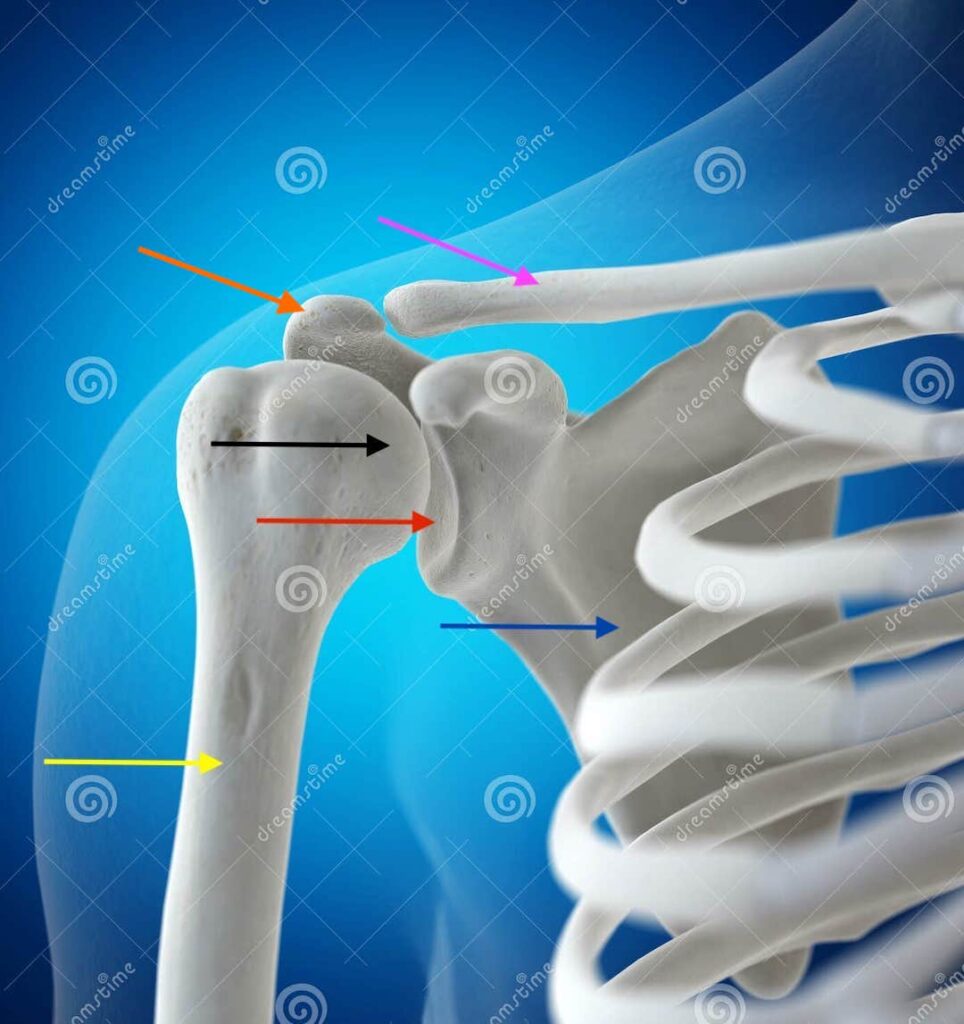
To understand what happened to Elspeth’s extremity and what Claire did to restore its normal anatomy and function, let us first examine the bones of the shoulder joint (next image).
Using arrows:
-
- Pink: right clavicle (collar bone)
- Blue: right scapula (shoulder blade)
- Yellow: right humerus (upper arm bone)
- Black: head of humerus
- Red: glenoid cavity (socket for head of humerus)
- Orange: acromion (bony tip of scapula = point of shoulder)
Normally, strong ligaments, a joint capsule, and muscle tendons snug the humeral head into the glenoid cavity. The proper anatomical name for this is the glenohumeral joint.
Note: The glenoid cavity is shallow which allows greater mobility of the humeral head. Think of swinging your arm in a circle as in slow pitch. Unfortunately, this splendid anatomy sacrifices stability in favor of mobility.
An accident can force the humeral head out of the glenoid cavity resulting in a dislocated shoulder joint. Once this happens, it can happen again more easily because ligaments are stretched.
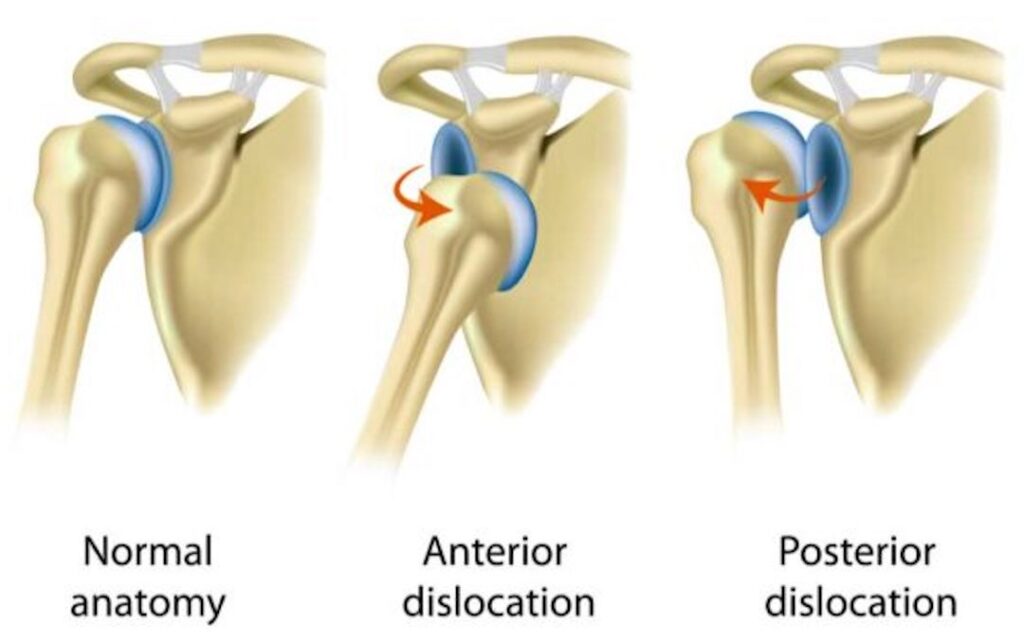
There are three types of shoulder dislocation. The next image shows two of the types plus a normal joint:
-
- Left: normal shoulder joint
- Middle: anterior dislocation (humeral head moves forward out of glenoid cavity)
- Right: posterior dislocation (humeral head moves backward out of glenoid cavity)
A third type is an inferior dislocation wherein the humeral head moves downward out of the glenoid cavity. This type is uncommon and is not shown in the diagram.
An anterior dislocation is most common and is the type suffered by Elspeth.
And…. let us nay forget! Jamie also suffered an anterior shoulder dislocation in Outlander episode 101!
Here, from Chapter 3, “The Man in the Wood.” of Outlander book:
I gasped, as did several of the men. The shoulder had been wounded; there was a deep ragged furrow across the top, and blood was running freely down the young man’s breast. But more shocking was the shoulder joint itself. A dreadful hump rose on that side, and the arm hung at an impossible angle.
In fact, I wrote a lesson about his injury waaay back in 2014 – Anatomy Lesson #2: Jamie and Claire Meet at a Joint”!

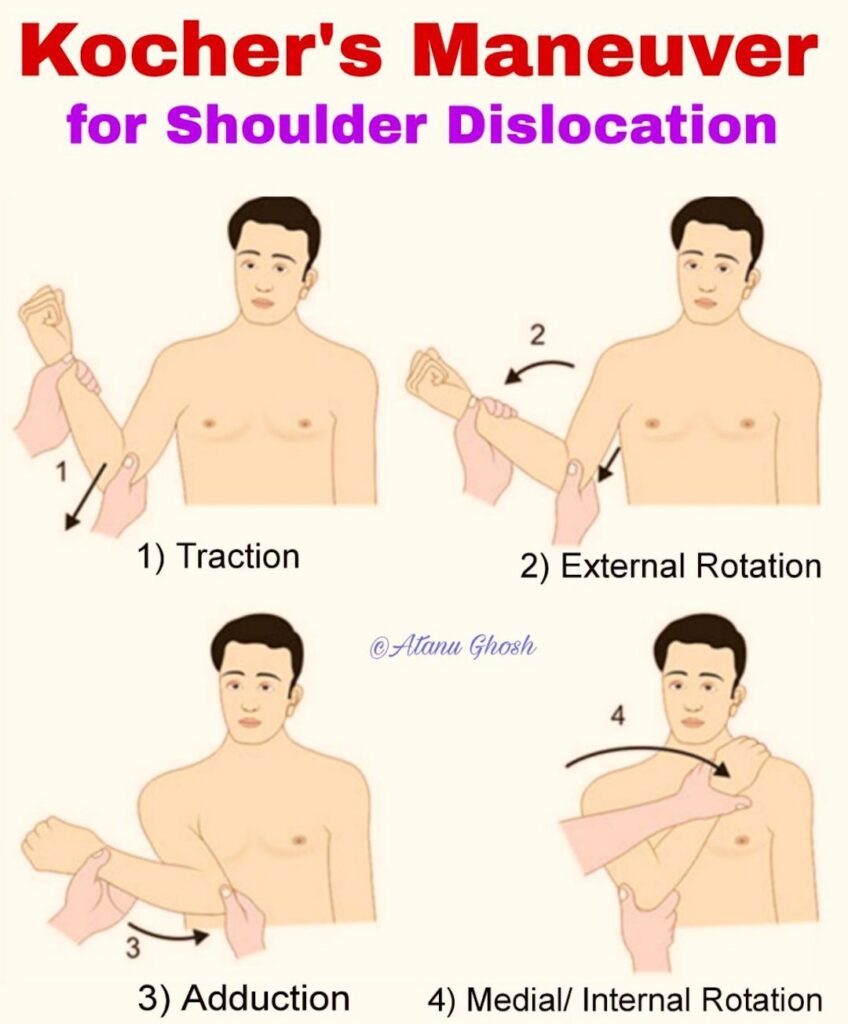
Claire reduces both Elspeth’s and Jamie’s anterior dislocations using Kocher’s reduction method. (Reduction means to return the dislocated extremity to its normal anatomy. )
Kocher’s method is typically broken down into the following steps (next image). But, first, the practitioner bends the elbow (flexion) gripping it with one hand and holding the wrist with the other hand. Then:
-
- Traction: The elbow is gently pulled toward the practitioner
- External Rotation: Hand and forearm are turned away from the torso (often slowly)
- Adduction: Elbow is moved against the torso
- Internal Rotation: Hand and forearm are turned across the chest
Swiss physician and Nobel Prize winner, Dr. Emil Theodor Kocher developed this technique in about 1890 and to this day, it remains the most widely used technique for anterior shoulder joint reduction.
(Pssst….You can see short videos of the Kocher method on a patient by searching You tube) 👀
The great physician, Hippocrates, also had a method for shoulder reduction which consisted of the practitioner placing his heel in the armpit of the patient and pulling on the affected extremity as shown in the next image! 😵💫

Many years ago, my family enjoyed a vacation featuring water slides. My husband took a slide before me. As I slid into the pool at the bottom, he climbed out of the water with his right arm dangling. He limped to an upright pole, lifted up the injured arm with his good hand, grasped the pole and leaned back. This maneuver immediately popped the dislocated humeral head back into place!
What happened? His arm hit the slide on the way down and he suffered an anterior dislocation. The dislocation reduced rather easily because he acted quickly before swelling set in. Once the joint tissues swell, reduction is more difficult and painful. (Psst….This was actually a variation of the Hippocrates method – hubby is a physician) 😷
So, in summary, Elspeth’s dislocation was resolved successfully by our brilliant healer but it did little to curb her sour disposition! 😜
I hope you enjoyed reading about Elspeth extremity.
Moral to the story…. be wary of wayward settles!
Until next time…
The deeply grateful,
Outlander Anatomist
Follow me on:
-
- Twitter: @OutLandAnatomy
- Facebook: OutlandishAnatomyLessons
- Instagram: @outlanderanatomy
- Tumblr: @outlanderanatomy
- Youtube: Outlander Anatomy
Photo credits: Outlander Anatomy; Starz; Sony; www.as2.Ftcdn.net; ww.researchgate.net; www.thumbs.dreamstime.com





{kind=link}