Hallo the house!
Welcome all anatomy students. I haven’t posted a lesson for a while, but Outlander Season 8 has given me new material to plumb. 🤓
I thoroughly enjoyed episode 802, “Prophecies.” This busy episode was made all the more riveting by the steady and creative hand of Caitriona Balfe in her directorial debut. The woman is soooo talented! 👸🏻
One scene captured my immediate attention: Frances and Claire in the surgery scoping out a scope! A microscope, that is. 🔬
This clever scene swiftly covers a broad range of anatomical topics:
-
- Microscope
- Paramecia
- Stomach
- Mucous membrane
- Slipperiness
Let’s take a closer look at each of these topics because we want to learn as much anatomy as possible. 📚
Microscope: First up, let’s discuss that magnificent microscope through which Francis peers!
Claire’s scope is either an accurate model of an 18th century scope or it is truly from that era. This image below shows an 18th century microscope that is a very close cousin.
Scope out the arrows to learn more about the microscope! 🔎
-
- Red Arrow: Indicates the eyepiece lens; it magnifies the object being examined.
- Blue Arrow: Indicates the objective lens which adds more magnification of the object.
- Orange Arrow: Marks the optical tube (barrel). This directs light from the objective lens to the eyepiece lens.
- Green Arrow: A glass slide which holds a drop of fluid and the object(s) to be observed.
- Yellow Arrow: A mirror reflects light upward through the object and into the microscope. It can be adjusted to enhance the amount of light entering the scope.
Notice: Frances holds a knob at the right side of the optical tube. This is the focus control, used to move the optical tube up and down to accurately focus on the object. 👁 The coarse knob is not visible on the scope in the image, below.
Both are compound microscopes, so named because two lenses are used to magnify an object; this is much more powerful than a single lens.
How it works: Light strikes the mirror and is reflected upward through the slide and the objective lens, into the optical tube and through the eyepiece lens. It then enters the eye creating an image on our retina of whatever is on the slide. That image is transferred as electrical signals to our visual cortex where we actually “see” the image. We do not see the image in our eyeball. 😮
Please note the candle flame in front of Claire’s microscope (above image). This provides light to the mirror. However, because there is a huge window to Frances’ left, I would skip the flame and turn the mirror to collect more visible light from the outside window! 🪟

Paramecia: Frances spies slipper-shaped creatures wriggling in the drop of water. These beasties are paramecia (pl.). The dark fragments in the slide are likely organic matter from a stagnant pond where Claire undoubtedly collected her specimen.

Paramecia are unicellular (single cell) organisms belonging to the Protist group. Historically, paramecia were categorized as members of the kingdom of Animalia. This changed in 1969 when they were moved into a kingdom all their own, the Protists. Recently, due to in depth DNA analysis, Paramecia now reside in the Eukaryota Domaine along with other protists, fungi, plants and animals.
Paramecia live in fresh, brackish, and marine waters. Claire was correct, these creatures do not cause human disease so ingesting them does not make us ill, although plenty of other stuff in pond water can make us sick.
These wee creatures have been studied so widely in research labs and in biology classrooms they are sometimes called microscopic lab rats! This is why Claire uses them as a teaching tool for young Frances.
Stomach: Claire tells Frances that our stomach protects and supports us because it:
-
- Is thick-walled ✅
- Contains mucus ✅
- Secretes acid ✅
- Digests proteins ✅
Check, check, check and check! True on all counts. Claire is one smart lassie. 😇
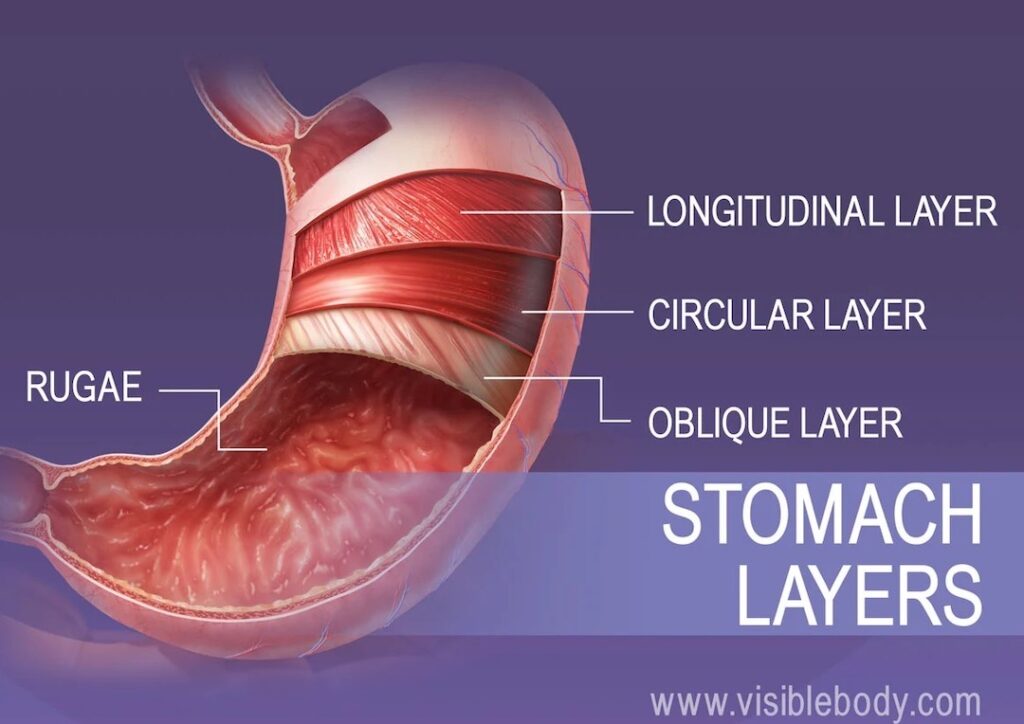
Most organs of the gastrointestinal tract have two layers of muscle in their walls but the stomach has three (longitudinal, circular & oblique), making it thick-walled, indeed!
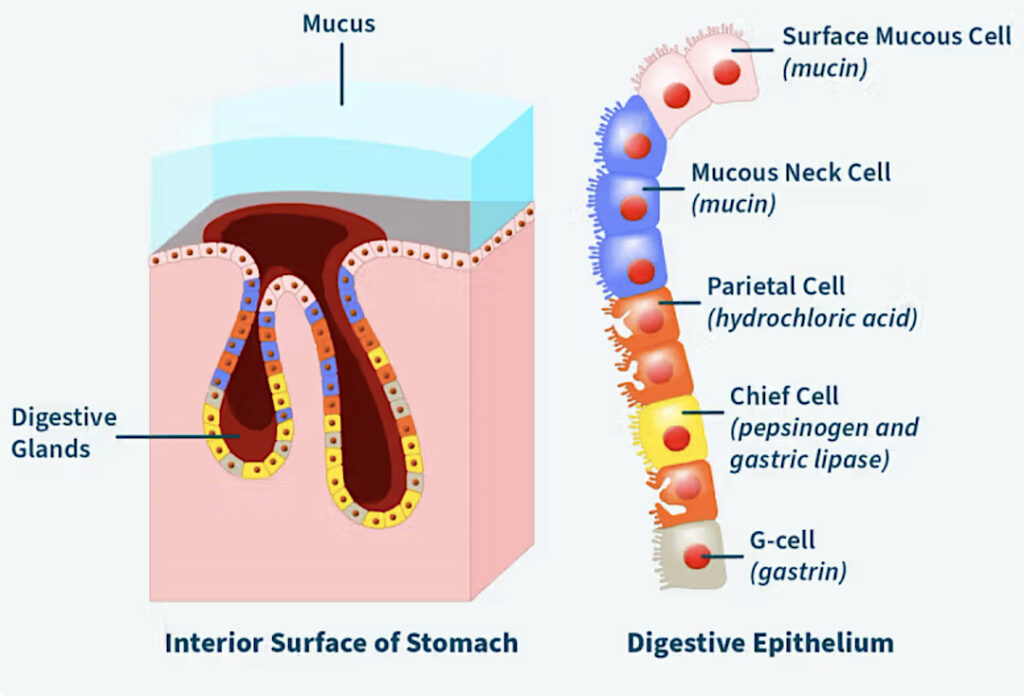
The stomach lining is indented with pits, all lined with countless cells. The next drawing depicts cells lining such a pit. Surface mucous cells and mucous neck cells produce mucus which flows onto the stomach surface.
Notice a difference in spelling? This is not an error. 😮 Mucus is the noun form and mucous is the adjective.
Claire scores again: mucus does help protect the stomach surface from irritating substances. It also lubricates the surface, provides immune defense, and aids in absorption.
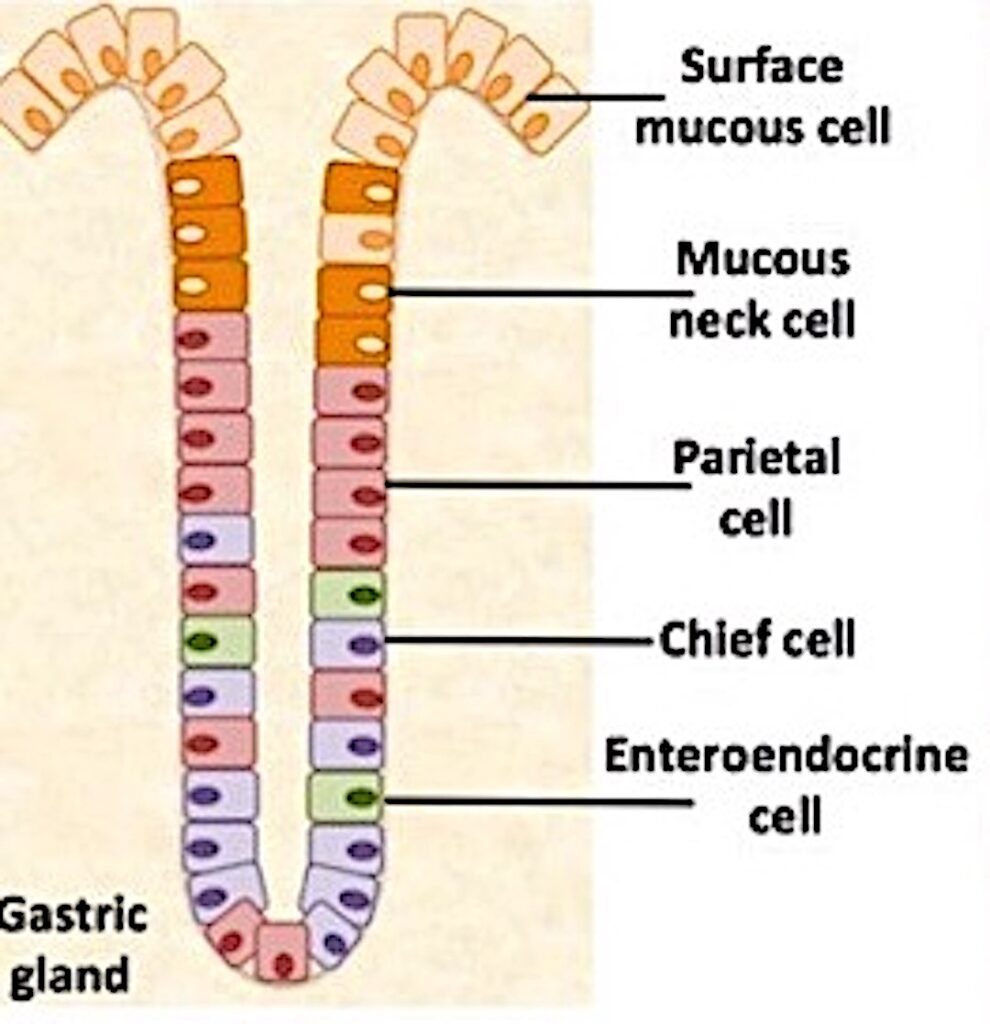
Another type of cell found deeper in the pits (next image), the parietal cell, (orange) produces hydrochloric acid (HCl). Our gastric HCl is a pH of 1-3, which is highly acidic. Just for perspective, the muriatic acid used to clean swimming pools is also hydrochloric acid! 😳
Little wonder we sometimes take an antidote to soothe an acid stomach? 💊
Lastly, the chief cell (yellow) produces an enzyme which along with HCl, alters and breaks down ingested protein.
Mucous Membranes:
Claire explains to Miss Frances that most of our organ are lined with mucous membranes. These surfaces are kept moist constantly by various mechanisms, a major one being mucus.
Mucous membranes are found throughout the gastrointestinal tract, respiratory tract, urinary tract, and parts of the reproductive tract. Even our conjunctivas and middle ears contain a few mucus-secreting cells. Mucous membranes are so ubiquitous that the average body contains roughly 2,153 sq ft of mucous membrane, roughly the same square footage as many homes!
The name, however, is unfortunate because not all mucous membranes produce mucus. Go figure! 🤔 An alternative name for mucous membrane is mucosa, a term I prefer because it doesn’t automatically imply that a given mucous membrane produces mucus.
Slipperiness:
“Snot? My stomach is full of snot?” Frances glances down at her tummy. “Well, yes,” says Claire.

Claire then explains how mucus helps our bodies be slippery when and where needed. For example, to help during the birth of a baby.

Oops! This is where Claire’s lesson goes a wee bit off the rails. 😉
You see, the vagina (birth canal) has no mucous cells or mucous glands of any kind in its structure.
Wait! What? My students were invariably astounded by this bit of science. But, this is why I love science and not opinion. Just because two bodily fluids are sticky does not mean are both are mucus.
For example, the vaginal fluid during sexual arousal is a slippery, protein-rich transudate produced by engorged blood vessels; it is not mucus! Ditto, the vaginal slipperiness during childbirth relies on this same vaginal transudate. 😎
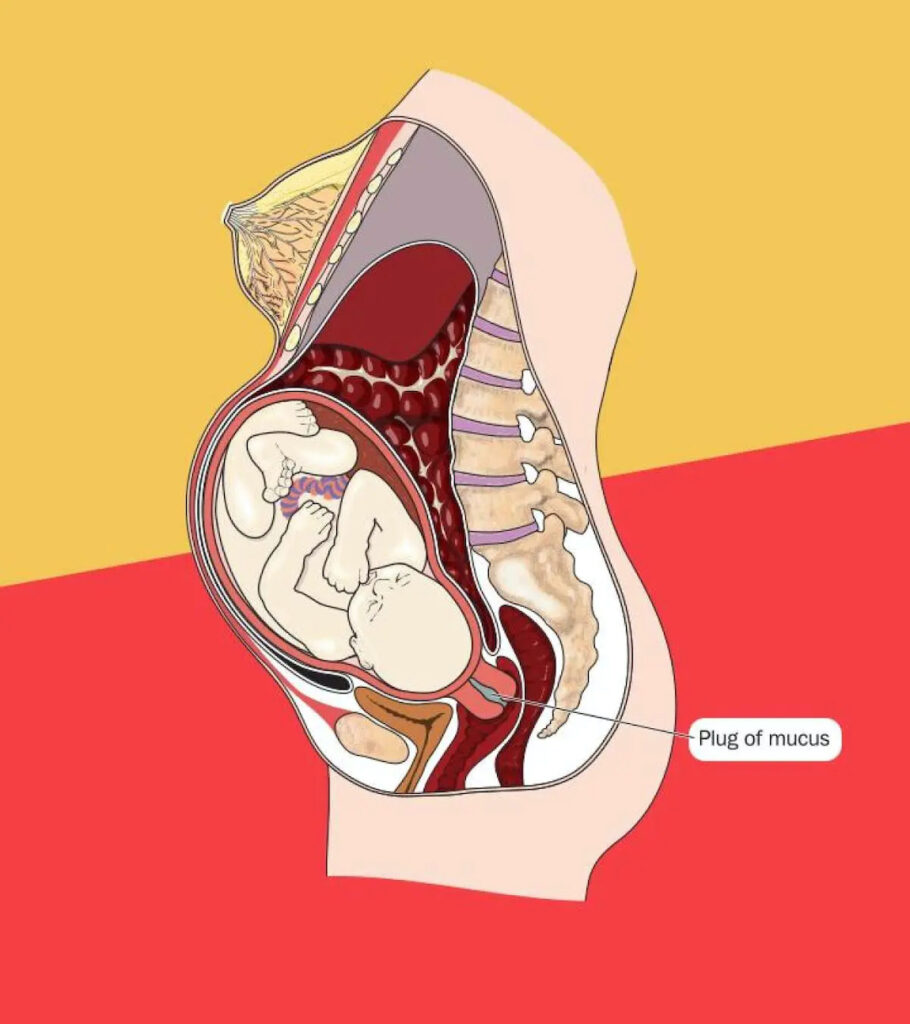
So, is there no mucus in the female reproductive tract? Well, there is some. The uterine lining produces some mucus. In fertile women, the uterine cervix produces a mucous plug (CMP) that stays intact until mid-cycle when it becomes more watery and penetrable by spermatozoa. During pregnancy, the CMP prevents vaginal bacterial from entering the uterine cavity.
There are also some mucous glands (Bartholin’s) near the external opening of the vagina that help moisten the area between the vulva. But, to reiterate, the vagina does not produce mucus.
Again, if no significant mucus is present, what causes vaginal slipperiness during childbirth?
This is how it works: Amniotic fluid, that surrounds the fetus, is a complex mixture of maternal fluid, fetal urine, nutrients, antibodies, hormones and fetal cells. Roughly one tablespoon of mucus from the CMP (0.03%) joins the amniotic fluid and together is normally discharged as childbirth approaches. But, the amniotic fluid often totally evacuates before labor even begins.
The slipperiness of the birth canal comes from those proteins of the vaginal transudate. And, yes, this slipperiness does help during childbirth (as well as during intercourse).
Just so you know, the CMP in post-menopausal women disappears due to lack of hormonal support. However, HRT (hormone replacement therapy) can restore the CMP in older women.
Other than this wee issue, Claire does a lovely job of explaining numerous biological details to a Frances, a wide-eyed and grateful student! 👀
Hang in there, Frances, I am sure there will be much more to learn from Dr. Claire. Jane would be proud!
I hope you enjoyed scoping out the scope, today. Watch for another lesson soon!

The deeply grateful,
Outlander Anatomist
Follow me on:
-
- Twitter: @OutLandAnatomy
- Facebook: OutlandishAnatomyLessons
- Instagram: @outlanderanatomy
- Tumblr: @outlanderanatomy
- Youtube: Outlander Anatomy
Photo credits:
Outlander Anatomy; Starz; Sony; www.Alamy.com; www.medline.gov; www.vmicro.iusm.iu.edu; www.momjunction.com; www.ourcancerstories.com; www.visiblebody.com;