Anatomy Def: An abdominal aortic aneurysm (AAA) is a bulge or swelling of the aorta that occurs in the belly.
Outlander Def: Mrs. Wilson’s untimely #death-resurrection-death wherein “kindly” fisher folk put Claire firmly on her witchy broom!!! 

Hello, anatomy students! To date, I have not written a full lesson about the cardiovascular (CV) system. So, the following quick anatomy lesson of the aorta will be useful in understanding AAA. 
And, we’re off!!! 
Aorta: The aorta is the largest blood vessel of the body! 
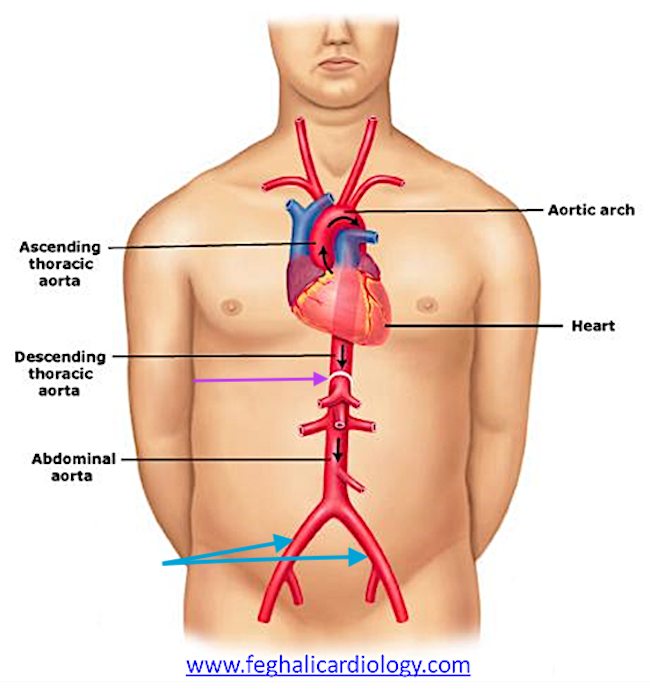
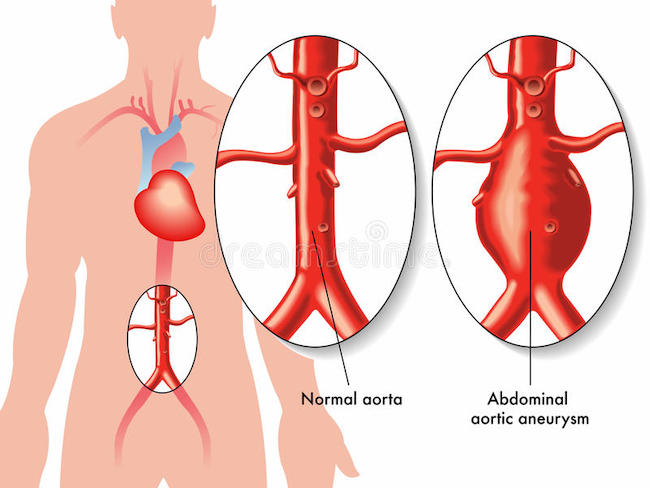
What Does it Do? The aorta is an artery, so it is tasked with carrying oxygen-rich (oxygenated) blood from the heart to general regions of the body. The direction of blood flow is indicated by the small black arrows in the next image.
Also, by convention, arteries are colored red to indicate these vessels carry oxygenated blood away from the heart and veins are blue to show vessels carrying oxygen-poor (deoxygenated) blood toward the heart. (pssst…there are two exceptions to this pattern, but I won’t confuse you by including those.  )
)
Along the entire course of the aorta, various arteries branch off to supply blood to the head and neck, upper limbs, chest and its organs, abdomen and its organs, and lower limbs. These branches are not labeled in the image below.
Divisions: Inside the chest is the thoracic aorta – the part within the belly is the abdominal aorta. The names switch where the aorta traverses the thoracic diaphragm (purple arrow).
The part of the thoracic aorta that rises is the ascending thoracic aorta, the curved part is the aortic arch, and the part that descends is the descending thoracic aorta.
Pathway: The aorta starts at the left ventricle (chamber) of the heart, rises toward the neck, makes a 180º, descends through the chest, and enters the belly (abdomen) where it terminates at the 4th lumbar (L4) vertebra by dividing into left and right common iliac arteries (turquoise arrows). Whew! 
How can a practitioner locate L4 when looking at the belly?
Here’s how: the umbilicus (navel) can be used as a fairly reliable surface landmark for termination of the aorta because it lies slightly above L4. Thus, a finger’s width below the navel will locate L4. If a person is heavy or pregnant, this can distort the position of the navel.
L4 is important because the practitioner must palpate above that level to detect a AAA.
Like other larger arteries, a pulse in the abdominal aorta can be felt (palpated). Sometimes the belly can be seen to rise and fall with the pulse especially after a meal, during pregnancy, or while lying down. This can be perfectly normal.
However, sometimes a pulse in the abdominal aorta can be a warning sign!
Aneurysm: If the aortic wall becomes damaged, it can developed a distinct bulge or balloon; this is an aneurysm. (Pssst… Aneurysms also can develop in smaller arteries and in veins.)
Aneurysms also can develop in smaller arteries and in veins.)
If an AAA is present, a practitioner may be able to detect the enlargement by palpating the abdominal wall. The care giver must press firmly enough to feel the abdominal aorta because it lies very deep, near the vertebral column.
If a patient has a very taut abdominal wall (next photo) or the waist girth exceeds 100 cm, it is more challenging for the practitioner to accurately feel and identify any aneurysm that may be present. A tight wall or a fairly thick layer of belly fat inhibits the deep pressure required for the exam. Lastly, clothes worn by the patient may also impede effective palpation! 

Although the following informative video is designed to train students on how to palpate the abdominal aorta, it is easily understood by a lay person. This will give you an idea of how a pulse is felt and how an aneurysm is detected.
The big problem with AAA is it can enlarge to the point of rupture, allowing blood to seep into the wall of the aorta (dissecting aneurysm) or bleed into the abdominal cavity causing dangerous blood loss or even death.
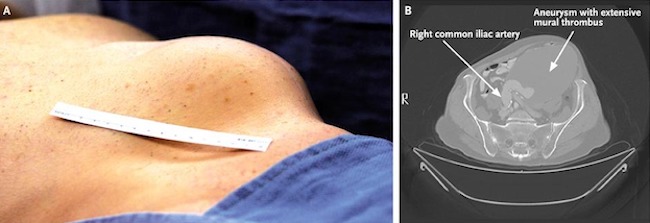
Rarely, an AAA can become so large, it is clearly visible in the abdominal wall (next image)! The left panel shows an huge bulge at the left side of a person’s abdominal wall. The right panel shows a cross-sectional CT scan of the same mass, identified as a huge blood clot (thrombus) in an AAA.
OK. I hear the bell tolling…… Time to head back to the wee kirk on the Ridge!
Germain’s “I spy with my little eye,” alerts Granny Fraser that something is amiss with Mrs. Wilson. 
“LOOK!“
“Stay back!”
Claire rushes to the other granny’s side and palpates her abdomen. Can she feel a possible aneurysm? Very likely, because Mrs. Wilson is fairly trim and her stays appear to be of the type that end near the waist, so Claire should be able to palpate – no problemo.
Claire slips her fingers between the folds of the skirt and takes a wee feel. Yep! Just as Claire suspected…..the auld lady has an abdominal aortic aneurysm – it has ruptured and she is bleeding internally.
If Mrs. Wilson had been sans clothes, Claire might have witnessed something like this:
She hasn’t got long, Reverend Roger. Just minutes and she stands before her Maker!

Wait! Wait! What? How could Claire ken the aneurysm had ruptured?
Well, here are some clues that Doc Fraser likely observed..….
Signs and symptoms that an AAA has ruptured:
-
- Sudden, intense and persistent abdominal or back pain – a tearing sensation
- Low blood pressure
- Loss of consciousness
- Pasty, cold, and clammy skin
Although Claire does not know if Mrs. Wilson experienced the back pain (no time to take a proper history), all the other symptoms are recognizable. Claire recognizes that given the lady’s advanced age, fainting is likely due to low blood pressure as a result of internal blood loss. Blood loss plus age suggest aneurysm as a likely cause. These coupled with palpation of the enlarged AAA leads Claire to tell Roger that Mrs. Wilson’s death is imminent! (She’s a lot closer to God than you, Roger Mac – Bree will be grateful for that  )
)
Mrs. Wilson revives long enough to forgive her SIL – “You’ve been a good lad.” He did provide her with a hame these past 20 years. ♥️

… And she survives long enough to accept the sin-eater’s gift of devouring her sins.
Lastly, you might be interested in what causes aneurysms and any risk factors.
Common Causes:
-
- Hardening of the Arteries (Atherosclerosis): Fat and other substances build up in the wall of the aorta (or other blood vessels) and weaken it.
- High blood pressure: Prolonged, elevated blood pressure can damage and weaken the aortic walls.
- Blood Vessel Diseases: Diseases such as Marfan Syndrome damage vascular walls.
- Infection: Although rare, a bacterial or fungal infection can cause AAA.
- Trauma: Abdominal injury (e.g. serious car accident) may cause an AAA due to a tear in the aorta.
Risk factors: And, like many other diseases, there are risk factors for AAA. Most of these we cannot control but there is one clear exception! 

-
- Tobacco use: Yep. Smoking is the strongest risk factor for AAA! Why? Because smoking weakens the aortic walls, increasing the risk of aortic aneurysm and the likelihood one might rupture. The longer and more one smokes or chews tobacco, the greater the chances of developing an aortic aneurysm. (Doctors recommend a one-time abdominal ultrasound to screen for an AAA in men ages 65 to 75 who are current or former cigarette smokers.)
- Age: AAA occurs most often in people ages 65 and older.
- Being male: Men are 3-4x more likely to develop AAA as women.
- Being white: People who are caucasian are at higher risk of AAA.
- Family history: Having a family history of AAA increases the risk.
- Other aneurysms: Having an aneurysm in another large blood vessel, such as the artery behind the knee or thoracic aorta can increase the risk of an AAA.
Read about Mrs. Wilson’s walk through the valley of the shadow of death in A Breath of Snow and Ashes, Diana’s longest big book (1,152 pages)!
“No, Grannie! Look!”
I followed his outthrust finger, and for a moment, thought he was pointing at his father. But he wasn’t.
Old Mrs. Wilson had opened her eyes.
There was an instant’s silence, as everyone’s eyes fastened at once on Mrs. Wilson. Then there was a collective gasp, and an instinctive stepping back, with shrieks of dismay and cries of pain as toes were trodden on and people squashed against the unyielding rough logs of the walls.
“Give her a bit of air, please,” I said, raising my voice. The stunned silence was giving way to a rising murmur of excitement, but this quelled as I fumbled to untie the bandage. The room waited in quivering expectation as the corpse worked stiff jaws.
“Where am I?” she said in a quavering voice. Her gaze passed disbelievingly round the room, settling at last on her daughter’s face.
I, meanwhile, had been doing my best to check the old lady’s vital signs, which were not all that vital, but nonetheless fairly good for someone who had been dead a moment before. Respiration very shallow, labored, a color like week-old oatmeal, cold, clammy skin despite the heat in the room, and I couldn’t find a pulse at all—though plainly she must have one. Mustn’t she?
I put my own hand on her abdomen, and felt it instantly. A pulse, where no pulse should be. It was irregular, stumbling, and bumping—but most assuredly there.
See Hiram Crombie’s MIL and her final moments before leaving her mortal coil in Outlander, Episode 602, Allegiance. A verra poignant scene, indeed!
Gobs of grannies in this episode! 
The deeply grateful,
Outlander Anatomist
Follow me on:
-
- Twitter: @OutLandAnatomy
- Facebook: OutlandishAnatomyLessons
- Instagram: @outlanderanatomy
- Tumblr: @outlanderanatomy
- Youtube: Outlander Anatomy
Photo Credits: Starz, www.familydoctor.org, www.feghalicardiology.com, www.nejm.org, www.oxfordmedicaleducation.com
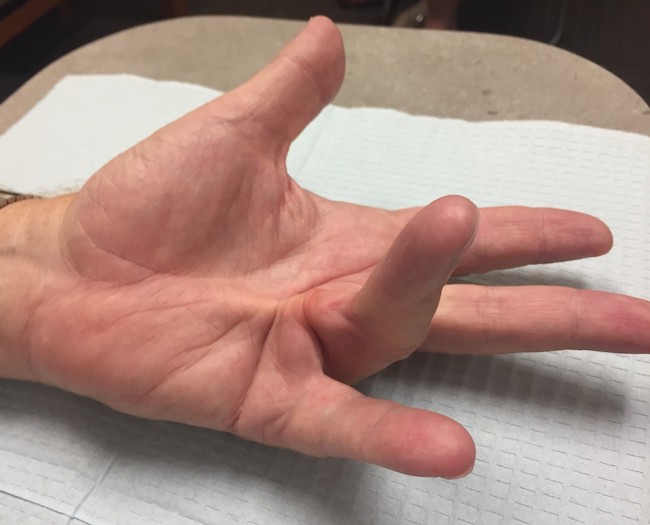
 Anatomy Def: Dupuytren’s Contracture, a disease involving changes to deep tissues of the palm.
Anatomy Def: Dupuytren’s Contracture, a disease involving changes to deep tissues of the palm.

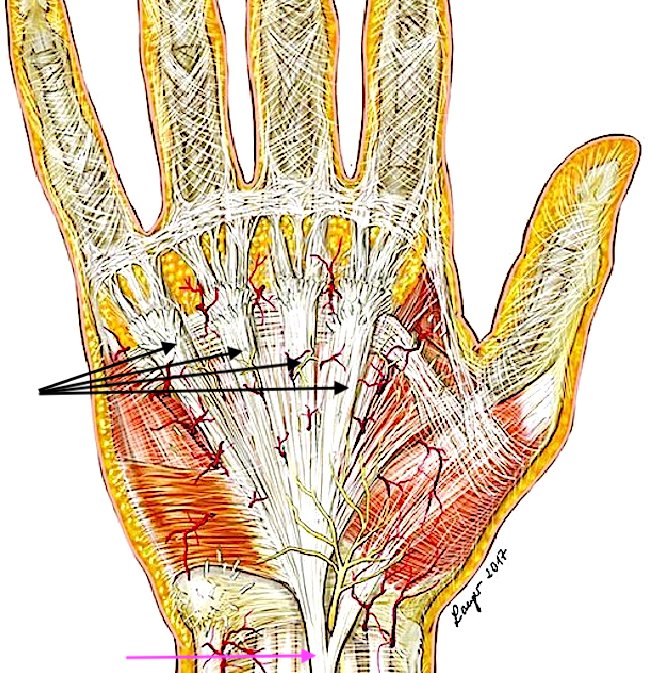

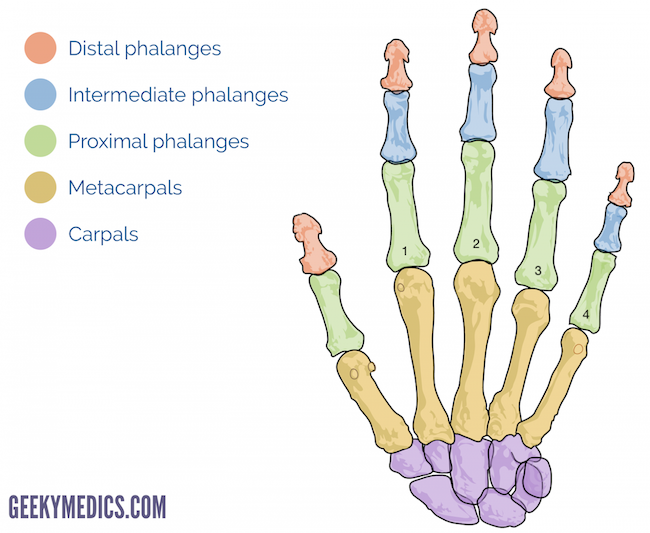
 Anatomists number fingers, from one to four:
Anatomists number fingers, from one to four: