Hallo, anatomy students. First lesson posted in a while – I have been waiting for new S4 material!
Meantime, “Me keep do.” So, here’s one last lesson from S3. Welcome to Anatomy Lesson #61, Jamie’s Mars and Scars!
Getting right to it…. Many events transpired in ep 306, A. Malcolm, wherein Jamie meets Claire after two hundred and twenty-two years apart. Woot!
Like you, the intimate scenes of this episode immediately drew my eyes to Jamie’s body – Oops, I mean his mars and scars. Come on, I’m a scientist!
My anatomist’s eye immediately began calculating… Weil, actually not until the second viewing, but you get my drift…. Are Jamie’s scars all present? Are any scars missing? Are they accurately depicted? Did they change?
What say you, Outlander fans, shall we investigate?
This is a chronological list of injuries over three seasons of Outlander TV and most produce scars. All but one appear in the books. Do you ken the outlier?
- dislocated shoulder joint
- gunshot wound, front
- gunshot wound, back
- BJR backlash
- McDonald’s sword work
- BJR hand smashing
- BJR burn
- BJR Culloden scar
Truly, this red-heided lad has suffered his share of owies!
We are all too aware of horrific wounds from modern warfare, but battlefield wounds have always been appalling. In the 16th century, French barber surgeon Ambrose Paré became famous for his ingenious repairs of battlefield injuries. One of his famous illustrations is a composite drawing that depictes the range of wounds suffered by warriors of the past (Image A). Seems as if our Jamie may have posed for this image. Gasp!
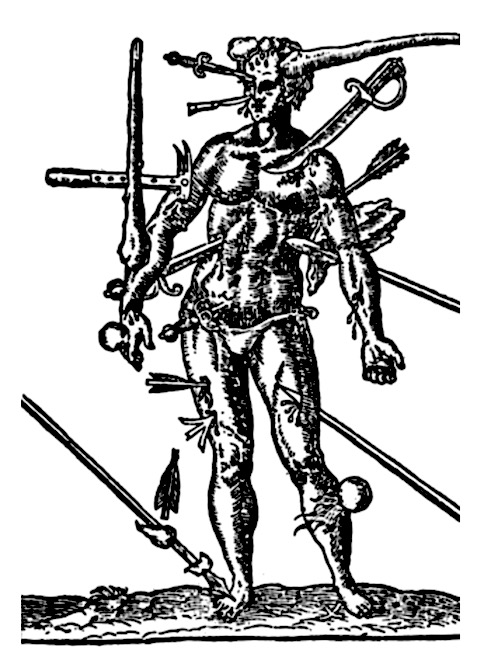
Image A
Just for fun and because you have nothing else to do <g>, let’s explore the laundry list of Jamie’s Wounds. We’ll jump backward and forward 20 years as we analyze his mars and scars in chronological order.
Strap yourselves in. Here we go!
1. Dislocated Shoulder Joint:
Claire first spies Jamie perched atop a stool in a crofter’s cottage (Starz ep 101, Outlander). His hunched form cradles right forearm. Her keen nurse’s eye is horrified by his injury. Here from Outlander book:
I gasped, as did several of the men. The shoulder had been wounded; there was a deep ragged furrow across the top, and blood was running freely down the young man’s breast. But more shocking was the shoulder joint itself. A dreadful hump rose on that side, and the arm hung at an impossible angle.
Q: What happened to Jamie?
A: He suffered an anterior dislocation of the right shoulder joint.
His fellow Highlanders move to force the joint into place but Claire-Declares, NO! No qualified chirurgeon in this grubby group of lads!
The dreadful “hump” is the acromion, a feature of the scapula (shoulder blade). Read about the shoulder joint and Claire’s treatment of its dislocation in Anatomy Lesson #2, When Claire Meets Jamie or How to Fall in Love While Reducing a Dislocated Shoulder Joint!
Footnote #1: In Outlander book, Jamie suffered both a dislocated shoulder and a gunshot wound. Diana wrote that the musket ball knocked him from the saddle and he fell on his hand. Crunch went the shoulder joint!

Outlander ep 101, Sassenach
Although bruising and swelling often accompany such dislocations, both may resolve without sequelae. Jumping forward 20 years, witness Jamie’s fine form at the brothel reunion in Starz ep 306, A. Malcolm. Evidence of a shoulder dislocation? Nada! Fortunately for Claire, this shoulder works perfectly fine. In fact, everything works perfectly fine. Wink, wink!

Outlander ep 306, A. Malcolm
Before we leave the shoulder issue, several fans have asked if the TV depiction of Jamie’s dislocation is realistic. Well, mostly. An actual anterior dislocation of the shoulder joint looks like Image B (left shoulder). Here, the rounded contour of the shoulder is lost because head of the humerus has been displaced forward into the armpit area (axilla). The bony knob (red arrow) is the acromion but, clearly, it is not as prominent as depicted in the TV version.
The difference can be explained because in the TV episode, the “dreadful hump” was a prosthetic applied to the top of Jamie’s shoulder. Thus, the hump sits higher and appears more prominent than in life. But, otherwise, kudos to the special effects team!

Image B
Moving on!
2. Gunshot Wound, Front:
Back to the crofter’s cottage! Hightailing it towards home, the Highlanders are ambushed by Redcoats at Cocknammon Rock. But, the English are swiftly dispatched. Hours later, Claire shouts:
“Stop! Help! He’s going over!”
Timber!!! – Jamie topples from his steed.
Claire swiftly discovers a gunshot wound. Jamie, why didn’t you fess up? Now, Claire must deal with a nasty hole left by a musket ball plowing a path through Jamie’s trapezius muscle! Claire explains to Dougal’s merry band of men (Outlander book):
“The gunshot wound has been bleeding again, and the idiot’s been knifed as well. I think it’s not serious, but he’s lost quite a lot of blood. His shirt is soaked through, but I don’t know how much of it is his. He needs rest and quiet; we should camp here at least until morning.”
Fat chance Dougal will stop for his nephew to rest; not with Captain Randall prancing through the heather.
“On your feet, soldier!”
Footnote #2: The TV version shifted the gunshot wound later in the episode and completely ignored the knifing. Probably figured Claire had enough on her plate. Hah!

Outlander ep 101, Sassenach
Fast forward 20 years: Delightful! Starz FX team remembered to include a faint scar as evidence of that entrance crater left by the musket ball.
Can’t you just see a Starz employee with a wound list?
- Dislocated shoulder joint, check!
- Front gunshot wound, check! (
- etc.

Outlander ep 306, A. Malcolm
3. Gunshot Wound, Back:
Back to the past. Next morning, in Castle Leoch’s keep, wary Claire meets-and-greets wary Mrs. Fitz – immortalized in this masterful excerpt from Outlander book:
“But he’s hurt. He was shot yesterday and stabbed last night. I bandaged the wound for riding, but I didn’t have time to clean or dress it properly. I must care for it now, before it gets infected.”
“Infected?”
“Yes, that is, I mean, inflamed, you know, with pus and swelling and fever.”
“Oh, aye, I know what ye mean. But do ye mean to say as ye know what to do for that? Are ye a charmer then? A Beaton?”
“Something like that.”
This terse little tête-à-tête, wherein WWII combat nurse and 17th century castle housekeeper face-off, reveals Claire’s nimble brain! The term infected, meaning invasion by micro-organism, won’t come into common use for another century. Oops, she quickly course-corrects!
Then, off she goes to properly tend Jamie. (One might think the lad is accident prone!)
The wound at back of shoulder marks the exit site of the musket ball. Serious bruising from gunshot wound and dislocated shoulder and horrific criss-crossing scars (see below) definitely catch her eye. Eek!

Outlander ep 102, Castle Leoch
Spring forward 20 years. Was the exit wound depicted at the brothel reunion? Aye, it was. Take a really close keek at Jamie’s back….there it be (red arrow).
Psst…let’s just ignore the unfortunate pleating of Jamie’s back prosthesis – best save those pleats for his kilt.
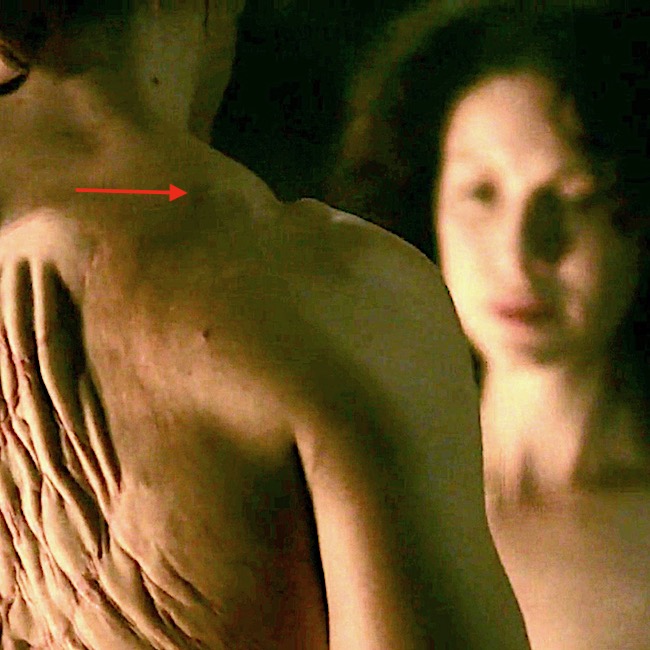
Outlander ep 306, A. Malcolm
Next!
Back to Castle Leoch. We can consider Rupert’s hearty beating of Jamie who gallantly choses fists over strap (enough straps) to protect loose-behaving Missy Laoghaire. Once again, mars are treated by Outlander Nurse. But, none of these blows caused permanent damage, so let’s move on!

Outlander ep 102, Castle leoch
4. BJR Backlash:
Just right for Hallowe’en – foul work by a foul one! Fast forward to ep 106, The Garrison Commander, wherein Captain Blackguard informs Claire of his beautiful masterpiece. Produced four years earlier, BJ floged Jamie’s back into a bloody mess using a cat-‘o-nine tails with lead tips. Yep, these do leave scars! And, dinna forget, Jamie already had been flogged days earlier! 😳
If you can stomach more flogging details, read Anatomy Lesson #10, Jamie’s Back – Aye, Jamie’s Back!
Described by Dougal in Outlander book:
Dougal grimaced. “A pitiful sight, it was, too—still raw, no more than half-healed, wi’ the weals turned black and the rest yellow wi’ bruises. The thought of a whip comin’ down on that soreness was enough to make me blench, along wi’ most of those watching.”

Outlander ep 106, The Garrison Commander
So naturally, the back scars persist two decades later.
A splendid quote from Voyager book; Jamie’s scars have healed and contracted as scars normally do.
I curled up behind him, knees fitting neatly behind his own. The firelight shone dully from behind me now, gleaming over the smooth round of his shoulder and dimly illuminating his back. I could see the faint lines of the scars that webbed his shoulders, thin streaks of silver on his flesh. At one time, I had known those scars so intimately, I could have traced them with my fingers, blindfolded.
Footnote #3: To my eye, the prosthesis at Madam Jeanne’s establishment appears identical to the original. Over a 20-year span, such scars should contract and thickness diminish. I suggest a new prosthesis to document these changes, an expected progression of wound healing and scar formation.
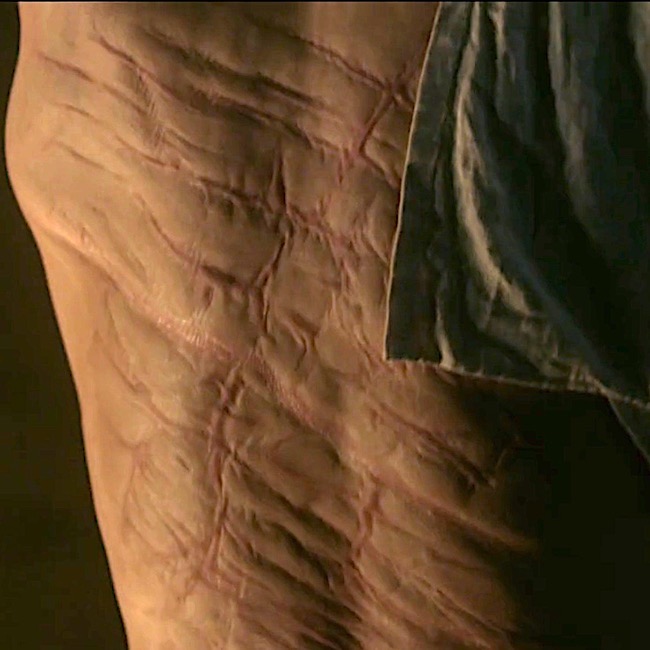
Outlander ep 306, A. Malcolm
5. MacDonald’s Sword Work:
Back to the early years. Ye ken the MacDonald clan with its three nasty-mouthed bros? Best ignore them, Jamie.
Nope. He gives them sass and in return, suffers a slice and dice Big Mac Attack! Three against one? No fair!

Outlander ep 110, By The Pricking of My Thumbs
The moral to this event is arguable, but consider something along the line of: dinna get mouthy with the MacDonald clan, especially if three well-armed laddies are against one!
But, Jamie exacts his revenge as he slices the hamstrings of one attacker, who from henceforth will hobble. And, who is cowering behind the tree? The cowardly Duke, who soon has a fate-date with The Godfather! Yes!!!

Outlander ep 110, By The Pricking of My Thumbs
Later, Claire stitches Jamie’s sword wound using the biggest needle she can find – royally POed! Most of you ken that she accidentally stuck that needle into “Jamie’s” skin during filming. Och! 😱
Footnote #4: If you chose this as the only injury not in the books, score! Although Diana didn’t write the MacDonald fight, Jamie does suffer a saber-slash at Prestonpans. Here from Dragonfly in Amber:
It was a saber-slash, slanting across the ribs. A lucky angle; straight in and it would have gone deep into the intercostal muscles between the ribs. As it was, an eight-inch flap of skin gaped loose, red beginning to ooze beneath it again with the release of pressure. It would take a goodly number of stitches to repair, but aside from the constant danger of infection, the wound was in no way serious.

Outlander ep 110, By The Pricking of My Thumbs
Did the Outlander FX team include the scar from the Sandringham kebby-lebby? Yep! There it is basking in Claire afterglow!
Outlander ep 306, A. Malcolm
6. BJR Smashing:
You ken about smashing pumpkins? BJR has his version, whacking Jamie’s hand with a mallet, smashing metacarpals and phalanges.
Read more about BJR atrocious pastimes in Anatomy Lesson #22, Jamie’s Hand – Symbol of Sacrifice!

Outlander ep 115, Wentworth Prison
Once again, Claire to the rescue! She stitches Jamie’s wounds and splints broken metacarpals and phalanges. Herself clearly explains the fate of Jamie’s paw after BJR’s maniacal ministrations (Outlander book):
I began to lose myself in the concentration of the job, directing all my awareness to my fingertips, assessing each point of damage and deciding how best to draw the smashed bones back into alignment. Luckily the thumb had suffered least; only a simple fracture of the first joint. That would heal clean. The second knuckle on the fourth finger was completely gone; I felt only a pulpy grating of bone chips when I rolled it gently between my own thumb and forefinger, making Jamie groan. Nothing could be done about that, save splint the joint and hope for the best.
The compound fracture of the middle finger was the worst to contemplate. The finger would have to be pulled straight, drawing the protruding bone back through the torn flesh. I had seen this done before—under general anesthesia, with the guidance of X rays.
 Outlander ep 116, To Ransom A Man’s soul
Outlander ep 116, To Ransom A Man’s soul
And, heroically repairs his mangled hand. Not a surgeon yet, but she did well!

Outlander ep 116, To Ransom A Man’s soul
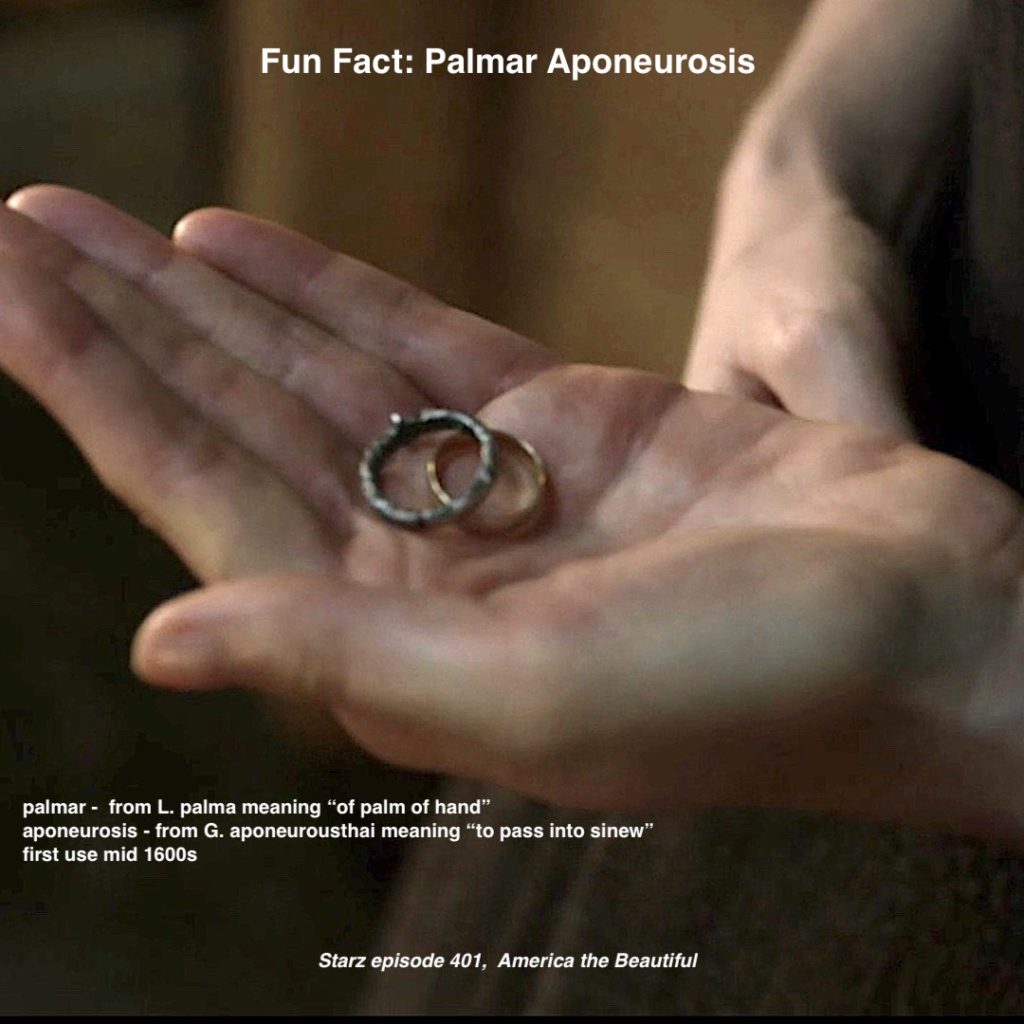
Are Jamie’s finger scars visible after 20 years? Oh, indeed they are! Look closely; nothing shows them better than eating grapes.
FX peeps were on their game. Plain as the back of your hand. Not that Claire was paying much heed to those scars, mind ye. Snort!

Outlander ep 306, A. Malcolm
7. BJR Burn:
Oh, and among those grim hours in the hands of a mad man, let’s not forget the ghastly image of BJR directing Jamie to burn initials into the flesh overlying his heart. Randall offers a red hot wax stamp to “seal” the job! Gah!

Outlander ep 116, To Ransom A Man’s Soul
Those initials do not survive because TV Godfather excises them and casts into the fiery pit. Go Murtagh! Rah!
Footnote #5: In Outlander book, Sir Marcus removes the offending button of skin:
“Best let me help ye, man. Ye’ll fall on it in a moment.” After a moment’s pause, Jamie reluctantly surrendered the knife and lay back against the wadded blanket. He touched his chest an inch or two below the nipple. “There.”
Sir Marcus reached to the sideboard and snagged a lamp, setting it on the stool he had vacated. At this distance, I couldn’t see what he was peering at; it looked like a small red burn, roughly circular in shape. He took another deliberate pull at his whisky glass, then set it down next to the lamp and pressed the tip of the knife against Jamie’s chest. I must have made an involuntary movement, because the Lady Annabelle clutched my sleeve with a murmured caution. The knife point pressed in and twisted suddenly, flicking away in the motion one uses to cut a bad spot out of a ripe peach. Jamie grunted, once, and a thin stream of red ran down the slope of his belly to stain the blanket.
Talk about branding! Deeply grateful, today’s entrepreneurs never met Johnathan Wolverton!

Outlander ep 116, To Ransom A Man’s Soul
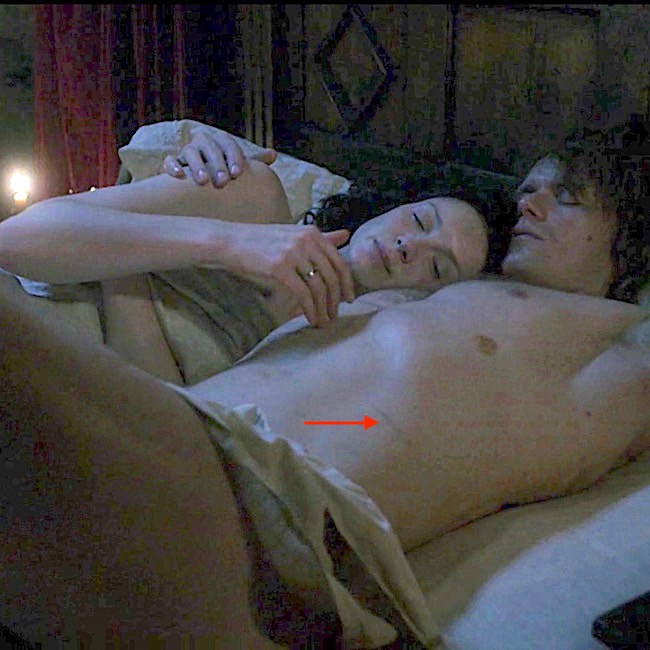
Back at the brothel, the burn scar is on full display (red arrow), looking a bit like a supernumerary nipple! He, he. The Starz crew didna forget!
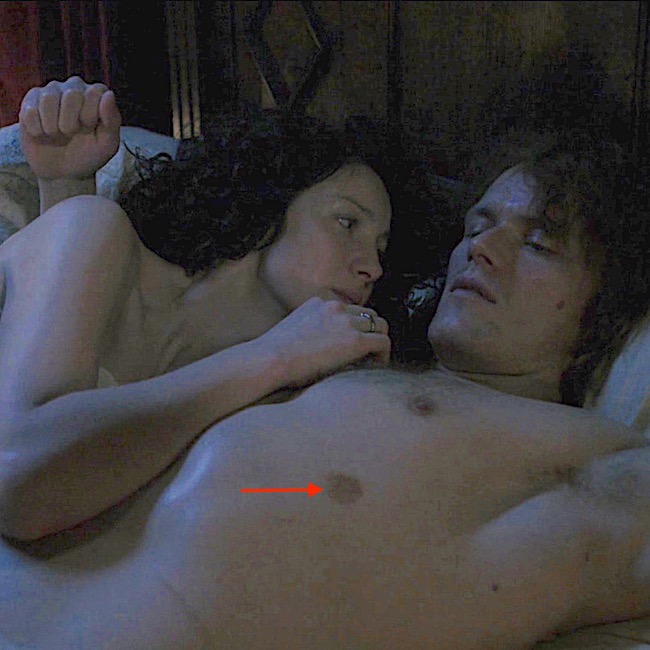
Outlander ep 306, A. Malcolm
And, finally, the last wound!
8. BJR Culloden Slash:
Black Jack is at it again – fiendish fiend! At Culloden, Jamie glances away from a fallen Randall and swish, the blackguard’s blade strikes and bites verra close to Jamie’s femoral artery!

Outlander ep 301, The Battle Joined
Twenty years later after the reunion-union, Claire espies the long thigh scar. Not quite as described in Voyager, but close. Outlander team snagged this one, too!
The scar ran from midthigh nearly to his groin, an eight-inch length of twisted, whitish tissue. I couldn’t repress a gasp at its appearance, and dropped to my knees beside him. I laid my cheek on his thigh, holding tight to his leg, as though I would keep him now—as I had not been able to keep him then. I could feel the slow, deep pulse of the blood through his femoral artery under my fingers—a bare inch away from the ugly gully of that twisting scar.
….Soft as a moth flying in the dark, my hand skimmed his leg, and found the thin deep runnel of the scar. My fingers traced its invisible length and paused, with the barest of touches at its end, wordlessly asking, “How?”
His breathing changed with a sigh, and his hand lay over mine.
“Culloden,” he said, the whispered word an evocation of tragedy. Death. Futility. And the terrible parting that had taken me from him.
Foot Note #6: In Voyager book, the scar extends to Jamie’s groin. The TV scar is closer to the knee – offering a modicum of modesty as millions take notice??? 😉

Outlander ep 306, A. Malcolm
So, eight wounds and FX folks nailed them all. Go team!
Think about it: BJ delivered almost 40% of Jamie’s wounds. However, if one counts each back scar, he owns well over 90% of Jamie’s mars and scars!
Oh, and here’s a wee bonus! Dinna forget loving Laoghaire’s contribution to Jamie’s landscape when the mad matron peppers him with bird shot. Of course, this event occurs after the reunion so those scars must await Season 4! Whew!

Starz ep 308, First Wife
Let’s close with this lesson with a snippet from big book seven, An Echo in the Bone, which aptly describes Claire as Jamie’s healer and helpmeet. Not really a spoiler as it reveals no plot points. So, safe to read.
A shadow fell across the floor in front of me and I looked up. Jamie was standing there with a most peculiar look on his face.
“What?” I said, startled. “Has something happened?”
“No,” he said, and advancing into the study, leaned down and put his hands on the desk, bringing his face within a foot of mine.
“Have ye ever been in the slightest doubt that I need ye?” he demanded. It took roughly half a second of thought to answer this. “No,” I replied promptly. “To the best of my knowledge, you needed me urgently the moment I saw you. And I haven’t had reason to think you’ve got any more self-sufficient since.

Outlander ep 308, First Wife
Final Points: Generally, society considers scars to be unwanted and unsightly. However, from anatomy and pathology POVs, scar formation is a normal process. Yes, indeed! This is the way mammalian creatures typically repair tissue disruption – like a biological bandaid. Although a scar may not perform as well as the original tissue, it keeps the body functional and responsive. To learn more about injury and repair, visit these anatomy lessons:
Recall the start of this lesson?
- Were all scars accounted for? Yes.
- Are any scars missing? No.
- Were they accurately depicted? Mostly.
- Did they change? Mostly.
Jamie’s mars and scars paint a poignant history. Claire was there for him from the get-go, treating broken bones, gunshot wounds, contusions, lacerations, incisions, dislocations, burns, and emotional abuse. Cheers to the gallant lass and her braw lad (and their creator)!
The deeply grateful,
Outlander Anatomist
Follow me on:
Photo Credits: Sony/Starz , adc.bmj.com (Image A); sghs.org (Image B)