
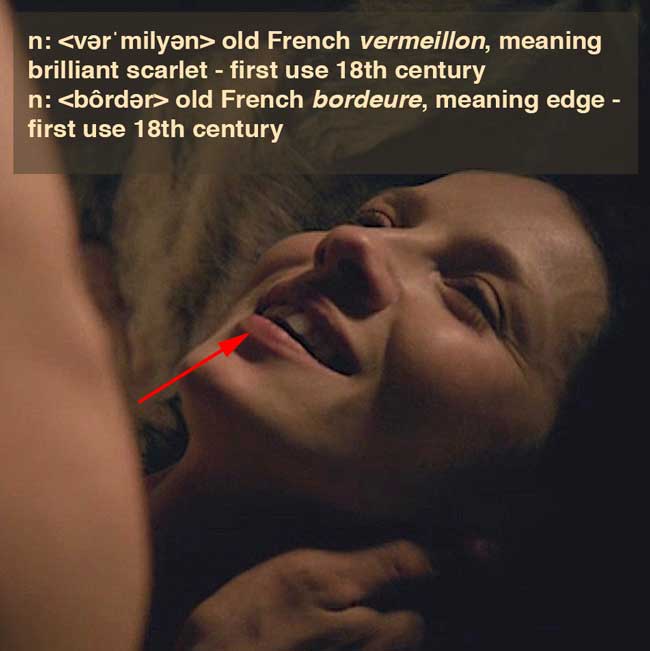
Anatomy def: Sharp demarcation (rim) where facial skin meets upper and lower lips (red arrow); the rim is often paler than the lips. Anatomical spelling is “vermilion,” not “vermillion.”
Outlander def: The perfect target for Jamie kisses! “da mi basia mille, diende centum, dein mille altera, dein secunda centum” … “Then let amorous kisses dwell, On our lips, begin and tell, A Thousand and a Hundred score, A Hundred, and a Thousand more.” (from Catullus – TY Diana!)
Learn about the vermilion border in Anatomy Lesson #14, Jamie and Claire – Anatomy of a Kiss.
Read about the edge (vermillion border) of Claire’s lips in Diana’s first book, Outlander. Gasp! Thud!
He reached out and touched my lower lip, barely brushing the edge. “It starts out the same, but then, after a moment,” he said, speaking softly, “suddenly it’s as though I’ve a living flame in my arms.” His touch grew firmer, outlining my lips and caressing the line of my jaw. “And I want only to throw myself into it and be consumed.”
See Claire’s lovely lips in each and every Starz episode, from season one through season two; but, Starz episode 107, The wedding, has particularly splendid examples! Claire’s exquisite lips are surrounded by a perfect vermilion border!
A deeply grateful,
Outlander Anatomist

 \
\