Greetings Outlander fans!
This is my final post about Surrey International Writers’ Conference (SiWC) held in Surrey, British Columbia on Oct. 25-27, 2024.
I had a fabulous time. Got to hear Diana perform in two workshops, one panel and Michael Slade’s Shock Theater. Great fun!
This last post is a review of Diana’s workshop entitled “Focus.”
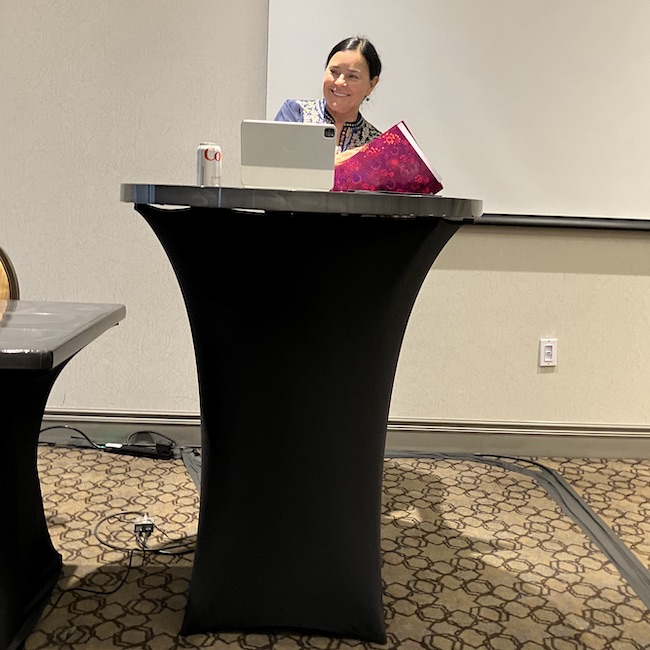
The room was filled to capacity even though it was the last day of the conference and some people had already left. This is an obvious testament to the respect she commands in the field of writing.
She arrived wearing a beautifully embroidered top and a lovely smile for all!
Diana began her workshop by explaining that she writes slowly because she considers every word she adds to her story.
She thinks book 10 will be her last Outlander book so she is putting a lot of thought into tying up loose ends both for her characters and various unresolved situations.
She also is working on a new Lord John book titled, ‘Black Chambers!”
She also wrote two scripts for the new Starz series, Blood of my Blood (BomB).
Of course, she also does numerous events, has a family and two grandsons which require a bit of her “focus,” too. This all helps account for her “slow” writing. 
Moving to the meat of her presentation, Diana learned early on how to get people to pay attention to what she wants them to pay attention to – this is the very definition of FOCUS! 
Next, she explained how using the five points of journalism helps a writer focus a reader’s attention by using:
As an example of focus, she read a new scene she has been working on. Will this excerpt appear in book 10, in the new Lord John book, or in another book? She does not say! 
Minnie, wife of Hal and sister-in-law of Lord John, is the main character in this scene. She stands on the deck of a ship. She has a letter in her pocket from her second son, Adam.
Diana informs the attendees that that Minnie is a character in “Fugitive Green,” originally a short story from “Seven Stones to Rise and Fall.” (Psst…..”Fugitive Green” is also now a stand alone novella!)
She starts by telling the reader who Minnie is: She is a woman that likes uncertainty! She has a conversation with Irishman, Raph (Raphael) O’Higgens, a character from “A Fugitive Green.” Then a whale arrives and the conversation focuses on the whale.
By the end of the scene, Diana has addressed all five of the journalistic points she discussed earlier!
She then explains several ways a writer can redirect a reader’s focus:
-
- Change the subject
- Create a loud noise
- Distraction by something outside the convo
- Add motion
- Add alliteration
- Use shiny objects

She then elaborates on why motion is so effective at changing focus. Humans are highly responsive to movement because we evolved as both predator and prey. Motion attracted our attention because it was a matter of life and death. 
She explains that a writer must also write. As an example, various Outlander cast members have asked for advice on how to write a book. She always recommends that they write for ten minutes every day for a week. By the end of the week they will know if they want to write a book! 
She also noted that Sam Heughan is the only cast member who did write a book – all the rest fell by the wayside when faced with her challenge.
Someone asked her how much research she did to write about the whale. She modestly answered that, well, she does have a Master’s Degree in marine biology so she knows something about whales. Big laughter!
She also read the whale chapter from “Moby Dick” which she found highly useful.
She noted that she made a big deal of the whale in this scene because a whale features later in whatever book this scene is destined to appear. 
She was asked about writing historical figures. Her rule is she tries not to make a historical figure do anything worse in her stories than the worst thing she knows about them! 
She pointed out that if you present the reader with a question, they want an answer, so don’t take too long to address it. (I will reiterate what I wrote in an earlier SiWC post….. Diana has made her readers sometimes wait 10 years and two books for answers!  )
)
She reiterated the three types of characters she writes. Most fans know these already:
-
- Mushrooms – characters that pop up, like Fergus
- Onions – complex characters with many layers, like Claire and Jamie
- Hard nuts – difficult to develop characters, like Bree
She also uses the rule of three…. For example, she always uses at least three senses to help the reader to focus and get into the character and what he/she is experiencing.
She believes she has a beneficial form of ADHD which has a huge impact on her writing and explains why she does not write in a straight line or follow an outline. Later, I asker her at lunch if she had been formally diagnosed and she has not but has read enough about the topic to deduct that it applies to her.
Diana ended her session by rereading a scene between Jamie and William. She has asked me not to share its contents. It is a very tender scene, I will say that.
The following is a recording of all of her workshop except that scene between William and Jamie – it was omitted. I hope you enjoy it.
Oh! There are 2-3 places where the recording is interrupted by extraneous noise. I think this was me shifting in my chair. I apologize. 

After the presentation, I gifted her with a bee-themed book bag. Inside is a small encaustic painting by my oldest daughter. Book readers will recall that book nine, “Go Tell the Bees that I am Gone,” has an entire chapter about encaustic painting.
All-in-all, Diana’s presentation was entertaining and enlightening. She always delivers useful information to the attendees and she does it with style and grace!
The deeply grateful,
Outlander Anatomist
Follow me on:
Video and Photo credits: Outlander Anatomy