Question #1: So, which is it, mold or mould? Ha, ha! Well, that depends on where you live. The entire English-speaking world, excepting the U.S., spells it, mould. Being somewhat contrarian, the US is the only English-speaking country that spells it, mold! 😉
Question #2: What is mold/mould? Molds are a large and diverse group of fungi (Pssst….. fungus is singular spelling, fungi is plural).
Question #3: What are fungi? In the past, fungi were classified as plants, but science marches on and fungi are now assigned to their own kingdom, placed on an even keel with plants, animals and two or three other kingdoms of life!
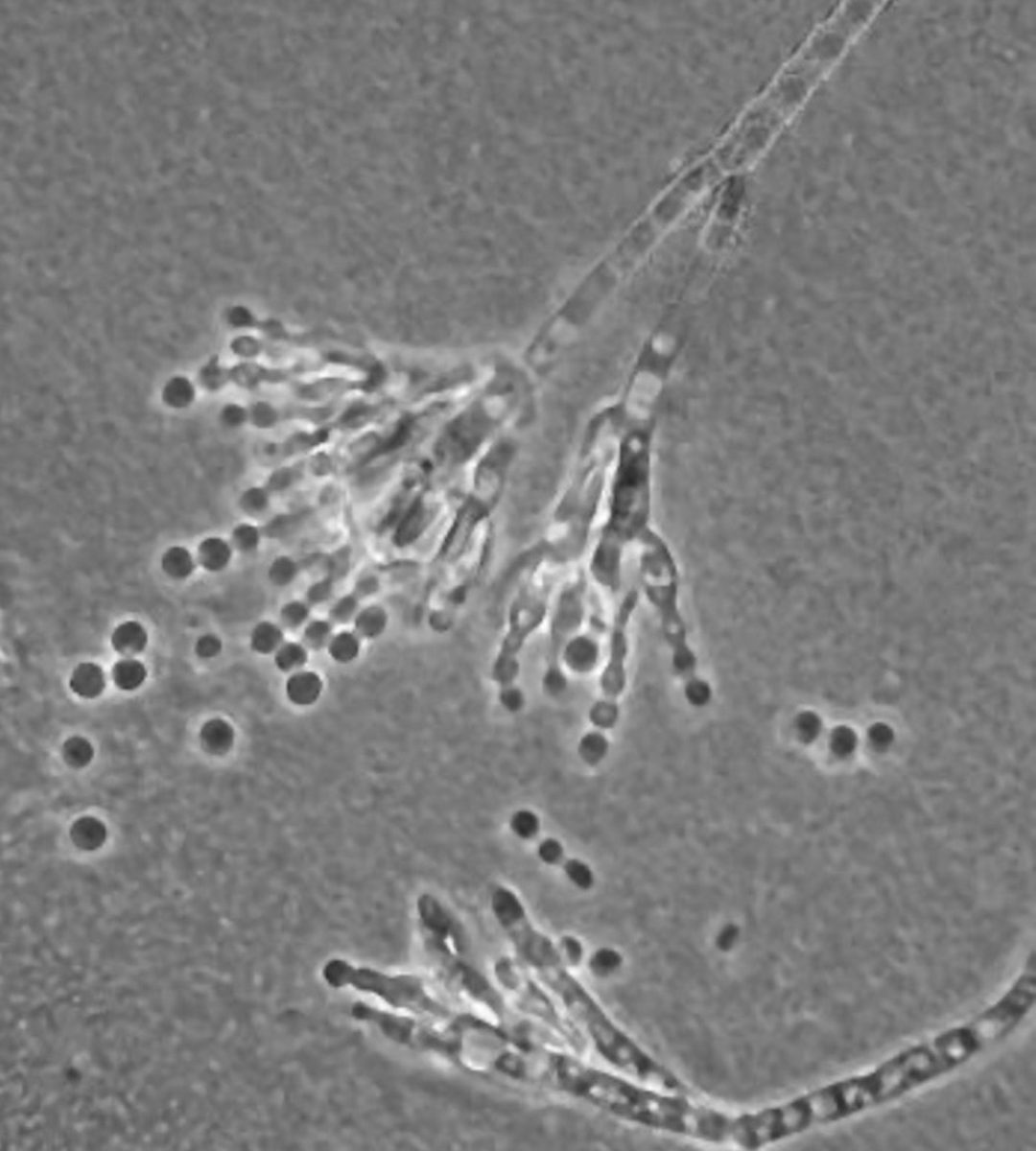
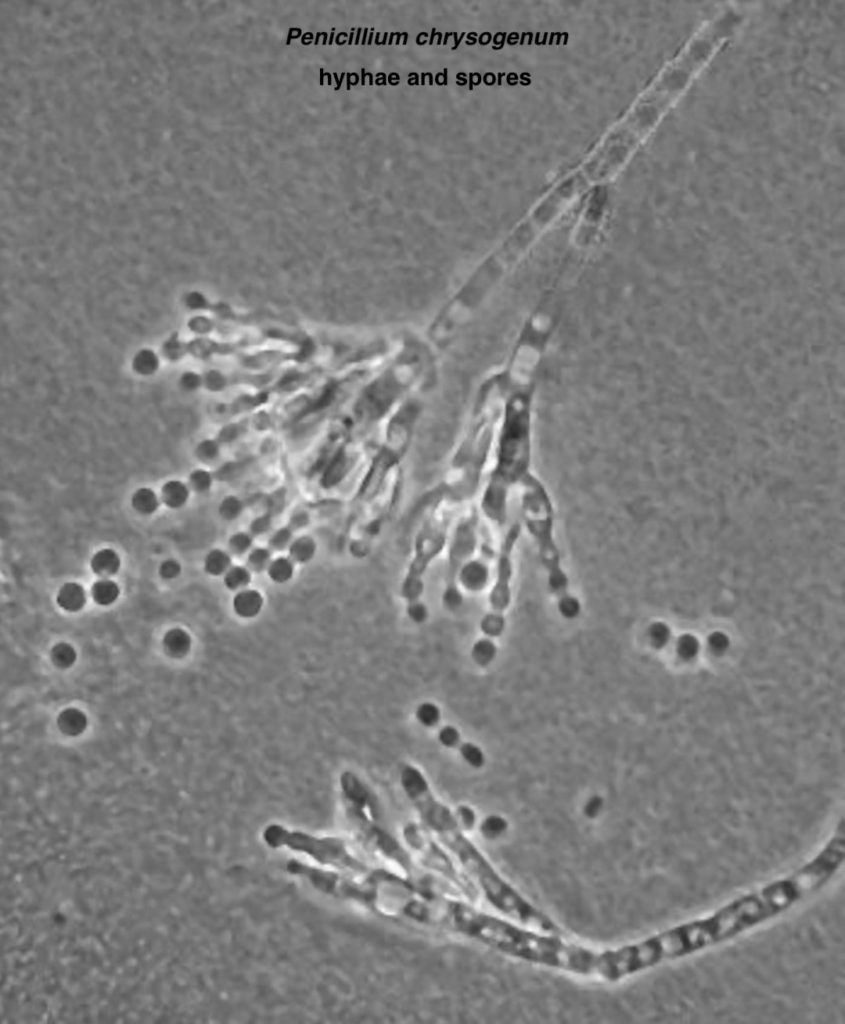
Mold Anatomy: Do molds exhibit anatomical features? Indeed they do! Molds grow by producing a network of transparent, branching tubules known as hyphae which lend molds their typical woolly-appearance. Molds also may have a dusty surface due to the production of spores at the tips of hyphae.
Claire kens that examination of spores and hyphae may help identify the type of mold she seeks; hence, experiments, microscope and Apprentice Marsali!
She seeks to grow a Penicillium strain that will provide a crude antibiotic. Claire, and now Marsali, will search for hyphae that look like wee paintbrushes in the microscope👇🏻! The small round globs are spores.
Let’s wish them the best of luck, although I do fash over Fergus’ recent paper grab; possibly a page of Claire’s lab notes? 😱
Spores act like seeds, a clever strategy to start new colonies. Mold spores released from parent hyphae are widely dispersed by:
air currents (can be airborne for long periods and distances)
fur
feather
clothing, etc.
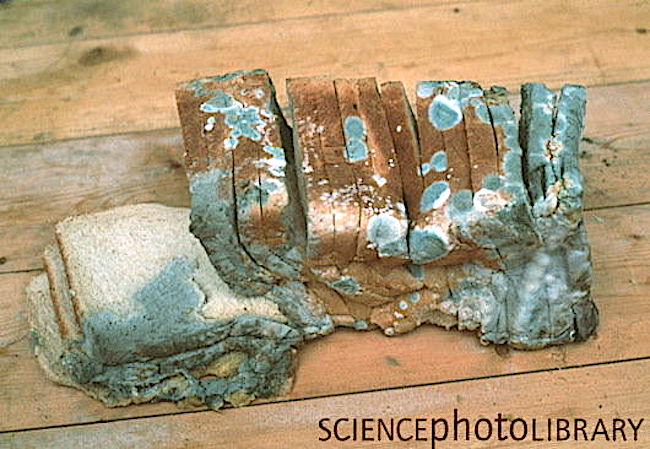
If spores land on organic material (e.g. chunks of homemade bread!) along with moisture, dim light, and warmth, they undergo cell division to produce the fuzzy molds our Sassenach seeks!
Fun Fact: Few molds will grow below 39 °F(4 °C) which is why refrigerators recommend settings around 38 °F. But, some hearty molds can survive Antarctica, acids, anti-bacterial soap, and jet fuel! 😳
Molds are a nuisance when they spoil food and damage property. They may also be pathogens causing allergies, invading tissues (e.g. lungs), or generating harmful toxins. On the other hand, molds are extremely useful in producing various foods and beverages, and by providing enzymes, pharmaceuticals, and antibiotics!
Read about Claire’s mold experiments in The Fiery Cross:
I twiddled the quill, rolling it between thumb and forefinger. I had kept a faithful account of my experiments with penicillin—the growing of cultures on media ranging from bread to chewed pawpaw and rotted melon rind, painstaking descriptions of the microscopic and gross identification of the Penicillium molds, the effects of—to this point—very limited applications.
Read the books, folks, wherein Diana faithfully details the mold experiments! 🙏🏻
See Claire’s bread mould/mold in Outlander episode 502, Between Two Fires. Yuck! 😝
Welcome, all students to Anatomy Lesson #58, Needles, Nerves and Penicillin. What do these words share in common? Why, Jamie, of course! In Anatomy Lesson #56, Achy Brachial Artery, we learned that birdshot from Laoghaire’s fowling piece almost ruptured one of Jamie’s major arteries. We also learned how Claire analyzed and repaired those wounds – based on human anatomy, of course!
Today’s lesson will examine Claire’s final cure for what ails her man. In Outlander episode 308, First Wife, we see her open a small medical bag equipped with needle, plunger and bottles of white fluid. What is she doing? Diana explains in Voyager book:
I laid the small, flat case on the table and flipped the latch. “I’m not going to let you die this time either,” I informed him, “greatly as I may be tempted.” I carefully extracted the roll of gray flannel and laid it on the table with a soft clinking noise. I unrolled the flannel, displaying the gleaming row of syringes, and rummaged in the box for the small bottle of penicillin tablets.
Translation: Dr. Claire busily prepares a hefty dose of penicillin for our fever-ravaged, red-heided hero! So, let’s begin the lesson with penicillin.
What is Penicillin? Penicillin is an antibiotic, from the English word, anti- meaning “against,” and the Greek word, bios meaning “life.” In a nut shell, antibiotics are substances which retard the growth of and/or destroy bacteria (germs).
How does Penicillin Work? First, understand that human cells are surrounded by a fragile cell membrane, but bacterial cells are surrounded by a sturdy cell wall. Penicillins destroy bacteria by preventing synthesis of said cell walls or by promoting processes to break them down. They do not harm human cells because our cells lack cell walls. Make sense? Grand!
From Whence Cometh, Penicillin: Before penicillin, there were no effective treatments for common infections such as pneumonia or rheumatic fever; hospitals were filled with folks suffering blood poisoning contracted from nothing more than a mere cut or scratch!
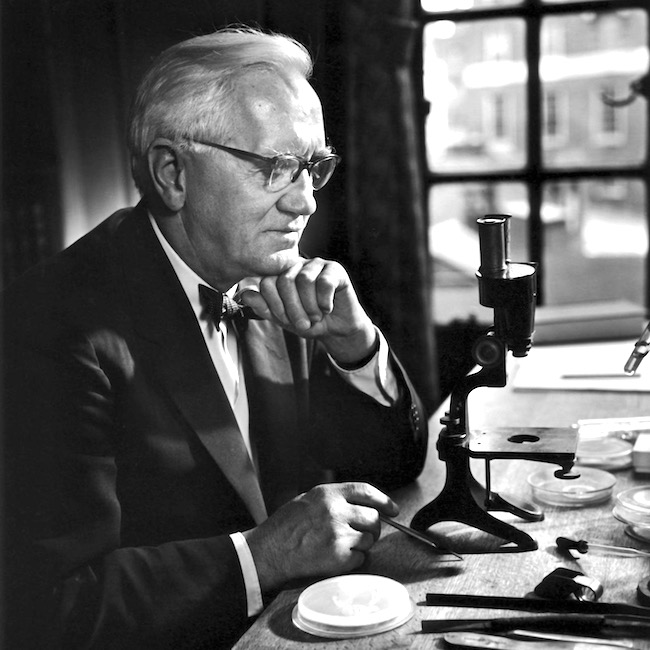
In 1928, Alexander Fleming (Image A), a British bacteriologist, returned from summer vacation in Scotland (yay!). Checking his lab specimens, he found that a mold (Penicillium notatum =P. notatum), probably from an open window, had contaminated his colonies of a common bacteria (Staphlococcus aureus or S. aureus).
Image A
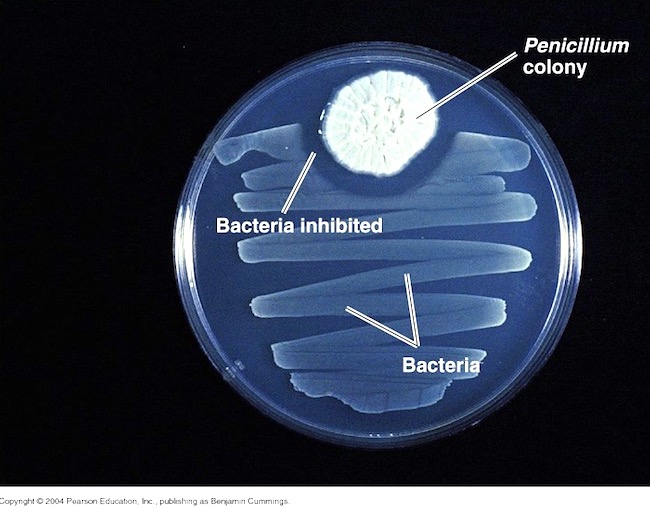
Examining the specimens via a truly primitive microscope (see Image A), he found the mold inhibited growth of S. aureus! Image B shows a modern version of what he observed: zigzagging ribbons of bacterial growth and a “halo” of no growth around the Penicillium colony. He correctly deduced his “mold juice,” which he later dubbed penicillin, inhibited bacterial growth!
Image B
Stop! Now, we might imagine this was an entirely modern discovery, but others in the early 1900s had made similar observations although not much came of these. Even more amazing? Ancient Egyptians applied a poultice of moldy bread to promote healing of infected wounds. Very doubtful that ancient Egyptian bread looked anything like this loaf of sliced, white bread (Image C), but you get the idea. Icky!
Image C
Penicillin to the Rescue! Fleming published his experiments in 1929, but his paper focused mostly on uses for penicillin in the lab with only a brief remark about possible therapeutic benefits.
Ten years later, an Australian scientist and Oxford pathologists proved penicillin was an effective antibiotic. But, the mold was cranky and fastidious to grown and the yield so low, only small quantities could be produced.
Enter WWII with its urgent need for battlefield antibiotics! Various pharmaceutical companies teamed with US Department of Agriculture to mass produce penicillin (the chemical engineer who designed 10,000 gal. production vats was a woman!).
Simultaneously, a global search was launched to find a new mold that could be grown easier and yield larger quantities of penicillin. One hot summer day, a laboratory assistant arrived with a cantaloupe covered in ”pretty, golden mold” which she (yes, another woman!) had found at a Peoria (IL) market. This mold was Penicillium chrysogeum, yielding 200 times the volume of penicillin as P. notatum!!! In 1954, using P. chrysogeum, US production of the drug jumped from 21 billion units to more than 6.8 trillion! And, penicillin was made available to allied forces (Image D).
A final note: Australia was the first country to make penicillin available for civilian use. Go, Aussies!
Penicillin does have drawbacks; it is ineffective against viruses and some types of bacteria (gram-negative), some people (0.03%) are allergic, and some bacteria have developed resistance due to over prescription or patients not following dosage instructions. Despite these drawbacks, penicillin can effectively treat the following short list of diseases (there is a long list, too):
Strep infections such as strep throat, scarlet fever
Staph infections such as post traumatic infections
Although I rarely move ahead of TV Outlander, this apropos quote from Diana’s book, The Fiery Cross,describes Claire’s work with penicillin. Herself wrote about molds from varied sources including the melon. Way to “break the mold,” Diana!
I twiddled the quill, rolling it between thumb and forefinger. I had kept a faithful account of my experiments with penicillin—the growing of cultures on media ranging from bread to chewed pawpaw and rotted melon rind, painstaking descriptions of the microscopic and gross identification of the Penicillium molds…
Nefarious Needles: With penicillin behind us (har, har) we broach the topic of needles. Ahhhh, yes, needles – a cruel device, with which most folks share a love-hate relationship! Claire prepares the penicillin and draws it into a syringe. Here, from Voyager book:
“What in God’s name are those?” Jamie asked, eyeing the syringes with interest. “They look wicked sharp.”
Psst … To me, he looks more wary than interested. Hah!
And more about needles:
I didn’t answer, occupied in dissolving the penicillin tablets in the vial of sterile water. I selected a glass barrel, fitted a needle, and pressed the tip through the rubber covering the mouth of the bottle.
Holding it up to the light, I pulled back slowly on the plunger, watching the thick white liquid fill the barrel, checking for bubbles.
And more!
Then pulling the needle free, I depressed the plunger slightly until a drop of liquid pearled from the point and rolled slowly down the length of the spike.
Claire’s penicillin is a thick, white liquid, poorly received by Jamie’s remarkably regal rump. We might ask, why Claire didn’t carry oral penicillin for her return trip to 1700s Scotland? It was available in her time. I really don’t ken the answer, but the injectable type promises readers and viewers a much more rousing and carousing tale! <G>
Understand, the first penicillins were injected, not ingested (Image E – puir wee laddie). Why? Because, when swallowed, stomach acid breaks down penicillin rendering it impotent. But, in the 1950s, types of oral penicillin which resisted stomach acid were developed. Today, many forms of penicillin include: capsule, chewable tablet, tablet for suspension, extended-release tablet, powder for suspension, powder for solution, capsule and syrup.
Image E
Claire also brought her own 20th century syringes because they had not been invented in Jamie’s time. Almost a century later (1840s), Irish physician Francis Rynd invented the hollow needle to deliver the first modern-era subcutaneous (under-the-skin) injections! …”I’ve Got You Under My Skinnn!” ? Och!
Before we move on, let us honor resourceful Pre-columbian Native Americans who created early hypodermic needles and syringes using “hollow bird bones and small animal bladders!” Incredibly inventive and creative – using only nature’s gifts to presumably administer healing substances! No Spoilers: This relatively unknown fact should please book readers who will recognize something similar which Claire employs in The Fiery Cross.
I’ve said it before and I’ll say it again: if you haven’t read/listened to the books, you are missing one long joyous, glorious voyage!
More penicillin adventures from Voyager book. Claire stabs Jamie in the backside with her wee needle spike. Hah!
“Roll onto your good side,” I said, turning to Jamie, “and pull up your shirt.” He eyed the needle in my hand with keen suspicion, but reluctantly obeyed. I surveyed the terrain with approval. “Your bottom hasn’t changed a bit in twenty years,” I remarked, admiring the muscular curves.
… I jabbed deftly and pressed the plunger slowly in.
“Ouch!” Jamie rubbed his posterior resentfully.
“It’ll stop stinging in a minute.” … Finally he said, “I thought ye stuck pins in ill-wish dolls when ye meant to witch someone; not in the people themselves.”
“It’s not a pin, it’s a hypodermic syringe.”
“I dinna care what ye call it; it felt like a bloody horseshoe nail. Would ye care to tell me why jabbing pins in my arse is going to help my arm?”
Splendid, splendid passage!
Here’s a few pearls from the above quote to consider: Why did Claire push the plunger slowly? Because, penicillin is a thick liquid which flows slowly and because it is viscous, it requires a large bore needle (18 gauge). The bigger the needle, the more it hurts while traversing the skin (yikes)! Because it is injected into muscle, the fibers are pushed apart by the fluid and that hurts, too! I well remember penicillin shots from my youth. Not fun!
Crucial Question: Let’s get to the bottom of things (snicker)…..is Claire free to poke that needle anywhere in Jamie’s bottom? Absolutely not!!! Clarie carefully selects the area where she deftly jabs her needle spike.
Anatomy to the Rescue: Now, wait just a sec! Why does it matter where Claire sticks the needle? After all, it hurts regardless, right? Let’s find the answer by studying anatomy of the backside.
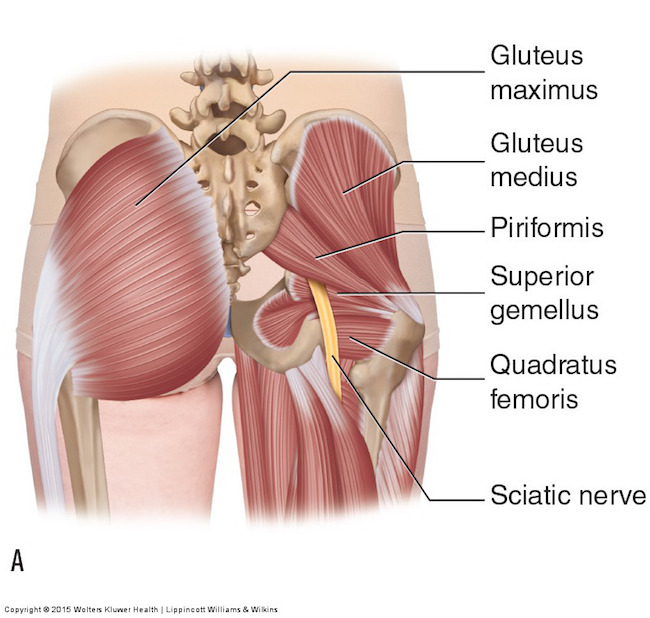
Remove skin and subcutaneous tissue and the buttock region looks like the left side of Image F: Each massive gluteus maximus muscle (Anatomy Lesson #1, Jamie’s Tush) covers the back of one hip. Because the muscle is thick and meaty, injection into its fibers is a perfect destination!
Try this: Stand erect and place your palms on each buttock with fingers facing downward. Now, clench your bottom and feel it lift and tighten (hopefully)? Gluteus maximus muscles at work!
Sciatic Nerve: Butt, wait (he, he)! Remove the gluteus maximus and what lies underneath (Image F – right side)? One sees a host of smaller hip muscles and a very large yellow structure emerging from under cover of the right piriformis muscle . This is the sciatic nerve, largest and longest nerve of the human body – many adult sciatic nerves are as big around as an adult thumb! And, just to keep us crazy, although most sciatic nerves emerge from below the piriformis, there are five other variations that occur with less frequency.
Each sciatic is formed by contributions from five levels of the spinal cord (L4, L5, S1, S2, S3 – Anatomy Lesson #10, Jamie’s Back or Aye, Jamie’s Back!) as it traverses one buttock and descends through the back of thigh. In case you don’t know, L = lumbar and S = sacral.
Image F
Protect the Sciatic Nerve! Heath practitioners who inject the buttock know this cardinal rule: Never inject penicillin (or other drug) into or near a nerve as this may result in permanent neurological damage! Such damage can include permanent paralysis, muscle inflammation, gangrene or necrosis (tissue death). Major arteries must also be avoided.
True Story: Years ago, I knew a woman with foot drop, meaning she could not lift her foot at the ankle joint (called dorsiflexion). Why? Because a careless health care provider injected penicillin into the wrong area of her gluteus maximus and it destroyed that part of the sciatic nerve responsible for innervating leg muscles which are required to lift the foot. And, yes, the injury was permanent!
Safe Zone: So, is there a safe zone for injections? Well, of course there is, otherwise, Claire would not have put her beloved Jamie at risk.
Let’s pretend this is Jamie’s bum. Hey, this is Jamie’s bum! <G> Black dots show regions corresponding to right and left buttocks. The blue rectangles are considered safe zones for intramuscular injections, including penicillin.
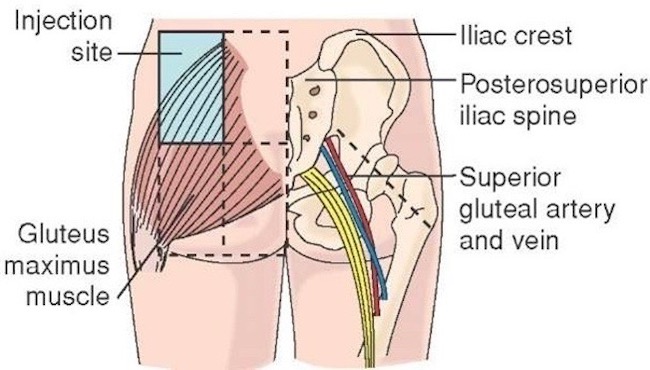
Using a graphic image might not be as much fun, but surely is informative. The buttock to be injected is divided into halves by a vertical line then divided into halves again by a horizontal line (Image G – left side). Injecting near the center of the upper outer quadrant, shown in blue, is considered the safe zone and avoids injuring sciatic nerve or nearby artery and vein (superior gluteal).
A newer technique uses a diagonal line as shown on the right side of Image G. Injecting above this line is also considered a safe zone. This line is harder to visualize because it requires a more thorough understanding of surface (topographical) anatomy.
Either technique is typically done in the mind’s eye of the practitioner, although, drawing actual lines on the buttock can also be done to verify safe zones.
Image G
This excellent You Tube video, created by Dr. Nabil Ebraheim, explains both approaches.
The meaty quadraceps femoris muscles (Anatomy Lesson #7, Jamie’s Thighs or Ode to Joy!) of the thigh present another acceptable site for penicillin injection. This explains why, much later on the Artemis, Claire injects herself in the thigh with penicillin after Jamie canna do the deed (Outlander episode 311, Uncharted). Our braw hero is afeared of wicked needles!
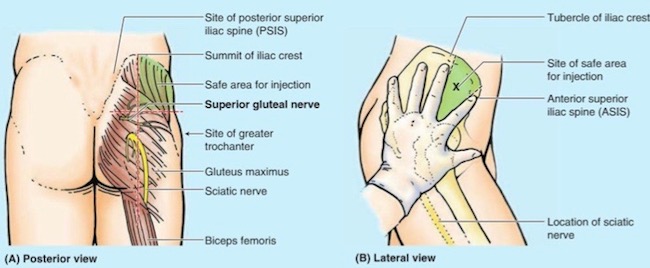
But, arguably the safest approach involves injecting into the gluteus medius muscle which peeks above the gluteus maximus. The safe region is indicated as the green area in Image H. This technique avoids the huge and very important sciatic nerve!
Ubiquitous Germs! One final issue and then our lesson ends. How might Jamie get an infection from second-wife wounds? Both birdshot and his skin would be likely sources for the bacteria causing his raging fever! Claire explains it quite well in this passage from Voyager book:
I took a deep breath. “Well, do you remember my once telling you about germs?”
He looked quite blank. “Little beasts too small to see,” I elaborated. “They can get into your body through bad food or water, or through open wounds, and if they do, they can make you ill.” He stared at his arm with interest. “I’ve germs in my arm, have I?” “You very definitely have.” I tapped a finger on the small flat box. “The medicine I just shot into your backside kills germs, though. You get another shot every four hours ’til this time tomorrow, and then we’ll see how you’re doing.”
I paused. Jamie was staring at me, shaking his head. “Do you understand?” I asked. He nodded slowly. “Aye, I do. I should ha’ let them burn ye, twenty years ago.”
Nay, Jamie doesn’t mean this wee salvo aimed at first wife. Snort!
Thank you Diana, Jamie and Claire for helping us to understand needles, nerves and penicillin!
Everywhere: Bacteria, molds and yeast are ubiquitous, covering virtually every non-sterile surface on earth. Recent tests have shown, seven of the 10 germiest (is this even a word?) spots in our homes are found in kitchens – with the dirtiest being kitchen sponges or dish cloths! Imagine, these are more germy than bathrooms!
Our lesson closes today with this visual of bacteria and molds found on one person’s hands (Image H). The hand was pressed into growth medium filling a petri dish. After some time, colonies of mold, yeast and bacteria grew from the hand print. Beautiful in an weird way, but definitely GROSS! The bottom line? Our mums were right. Let’s wash our hands!
Image H by Tasha L Sturm, microbiologist and photographer