This is my final post about Surrey International Writers’ Conference (SiWC) held in Surrey, British Columbia on Oct. 25-27, 2024.
I had a fabulous time. Got to hear Diana perform in two workshops, one panel and Michael Slade’s Shock Theater. Great fun!
This last post is a review of Diana’s workshop entitled “Focus.”
The room was filled to capacity even though it was the last day of the conference and some people had already left. This is an obvious testament to the respect she commands in the field of writing.
She arrived wearing a beautifully embroidered top and a lovely smile for all!
Diana began her workshop by explaining that she writes slowly because she considers every word she adds to her story.
She thinks book 10 will be her last Outlander book so she is putting a lot of thought into tying up loose ends both for her characters and various unresolved situations.
She also is working on a new Lord John book titled, ‘Black Chambers!”
She also wrote two scripts for the new Starz series, Blood of my Blood (BomB).
Of course, she also does numerous events, has a family and two grandsons which require a bit of her “focus,” too. This all helps account for her “slow” writing. 😉
Moving to the meat of her presentation, Diana learned early on how to get people to pay attention to what she wants them to pay attention to – this is the very definition of FOCUS! 🤗
Next, she explained how using the five points of journalism helps a writer focus a reader’s attention by using:
Who
What
When
Where
Why
As an example of focus, she read a new scene she has been working on. Will this excerpt appear in book 10, in the new Lord John book, or in another book? She does not say! 🤐
Minnie, wife of Hal and sister-in-law of Lord John, is the main character in this scene. She stands on the deck of a ship. She has a letter in her pocket from her second son, Adam.
Diana informs the attendees that that Minnie is a character in “Fugitive Green,” originally a short story from “Seven Stones to Rise and Fall.” (Psst…..”Fugitive Green” is also now a stand alone novella!)🤭
She starts by telling the reader who Minnie is: She is a woman that likes uncertainty! She has a conversation with Irishman, Raph (Raphael) O’Higgens, a character from “A Fugitive Green.” Then a whale arrives and the conversation focuses on the whale.
By the end of the scene, Diana has addressed all five of the journalistic points she discussed earlier!
She then explains several ways a writer can redirect a reader’s focus:
Change the subject
Create a loud noise
Distraction by something outside the convo
Add motion
Add alliteration
Use shiny objects 😄
She then elaborates on why motion is so effective at changing focus. Humans are highly responsive to movement because we evolved as both predator and prey. Motion attracted our attention because it was a matter of life and death. 😮
She explains that a writer must also write. As an example, various Outlander cast members have asked for advice on how to write a book. She always recommends that they write for ten minutes every day for a week. By the end of the week they will know if they want to write a book! 📖
She also noted that Sam Heughan is the only cast member who did write a book – all the rest fell by the wayside when faced with her challenge. 🤗
Someone asked her how much research she did to write about the whale. She modestly answered that, well, she does have a Master’s Degree in marine biology so she knows something about whales. Big laughter! 😄
She also read the whale chapter from “Moby Dick” which she found highly useful.
She noted that she made a big deal of the whale in this scene because a whale features later in whatever book this scene is destined to appear. 🐳
She was asked about writing historical figures. Her rule is she tries not to make a historical figure do anything worse in her stories than the worst thing she knows about them! 🤩
She pointed out that if you present the reader with a question, they want an answer, so don’t take too long to address it. (I will reiterate what I wrote in an earlier SiWC post….. Diana has made her readers sometimes wait 10 years and twobooks for answers! 😜)
She reiterated the three types of characters she writes. Most fans know these already:
Mushrooms – characters that pop up, like Fergus
Onions – complex characters with many layers, like Claire and Jamie
Hard nuts – difficult to develop characters, like Bree
She also uses the rule of three…. For example, she always uses at least three senses to help the reader to focus and get into the character and what he/she is experiencing.
She believes she has a beneficial form of ADHD which has a huge impact on her writing and explains why she does not write in a straight line or follow an outline. Later, I asker her at lunch if she had been formally diagnosed and she has not but has read enough about the topic to deduct that it applies to her.
Diana ended her session by rereading a scene between Jamie and William. She has asked me not to share its contents. It is a very tender scene, I will say that.
The following is a recording of all of her workshop except that scene between William and Jamie – it was omitted. I hope you enjoy it.
Oh! There are 2-3 places where the recording is interrupted by extraneous noise. I think this was me shifting in my chair. I apologize. 🙄
After the presentation, I gifted her with a bee-themed book bag. Inside is a small encaustic painting by my oldest daughter. Book readers will recall that book nine, “Go Tell the Bees that I am Gone,” has an entire chapter about encaustic painting.
All-in-all, Diana’s presentation was entertaining and enlightening. She always delivers useful information to the attendees and she does it with style and grace! 🤩
Good day, all! Apologies, this has taken a week to get to you! 😜
Sunday, October 9, was the final day of 2022 NYCC and, for me, it was the best!
Each morning walking to Javits, we were greeted by a “herd” of pigeons waiting for treats. Roomies, Jody and Jim, point to the feathered army! Usually, they were perched on the power lines reminding me of the 1963 Alfred Hitchcock film, The Birds! 😳
Inside the Javits, more cosplay.
Don’t know who this is but I’ll wager some of you do? It is a fab costume!
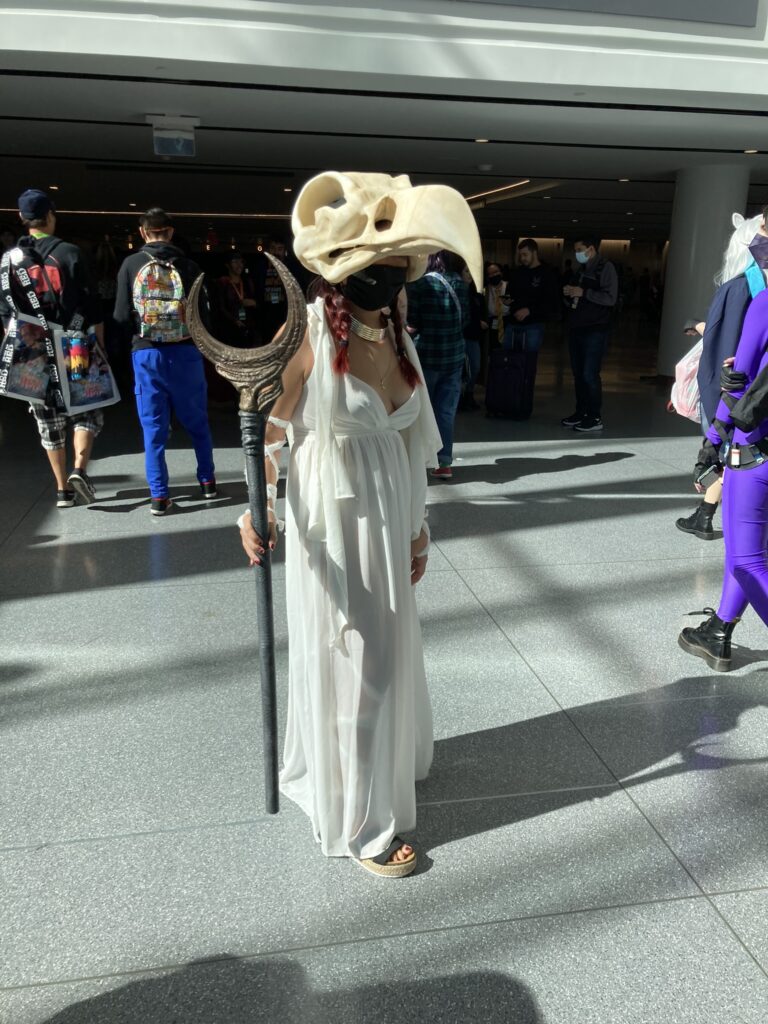
And, this intricate tableau…..
Anyone know? Wow! 😮
Onto the show floor where Jody quickly found her fav store, Tokidoki!
Next, Jody, Jim, and I were overshadowed by a huge Maga character!
Soon it was time to find a seat at the “Tea with Two Highlanders and A Lord” panel…. although, the title should have included “THE Lady.“
And, who might that be? Herself, of course! 🥰
I videoed the hour-long panel. My apologies for its homemade look. Occasionally, I had to switch hands and I also had to record most of it from the Jumbotron because I was too far back to capture a good stage view.
The panel was great and will speak for itself.
Enjoy!
(Psst….I never got any tea!) 😉
Afterward, the panelists retired behind the curtain for official photos. Then, as pre-arranged, Diana and her publicist emerged through a side door and I greeted her with a big hug!
She looked beautiful in her dramatic red cape, although this photo was taken sometime later. 😉 (It was a chill and windy day!)
I should mention, her splendid cape is made of warm wool with a tartan-lined hood. The sterling silver clasp appeared to be of Celtic design. I asked if it was from Scotland and she said, “I think so.” 😊
Pretty woman!
Then, we headed for lunch. It had been almost three years to the day since we shared a meal together and it was wonderful to see her again!
Her publicist took us down a private elevator to the basement of the Javits Center. I was intrigued by all the workings, supplies, and stuff in the “bowels of that building!” 😜
We hopped into golf carts and were escorted to the far end of Javits.
This is a video of our “zip ride.” You can hear me saying to Diana, it feels a bit like “James Bond.” 😆
We were driven to a door that opened street-side and walked to Hudson Yards to enjoy a quiet lunch.
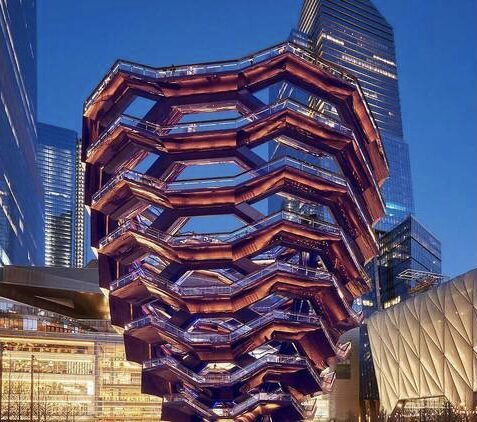
We took a moment to admire the beautiful ”Vessel” at Hudson Yards.
Fortunately, no fans took notice, and we snuggled in for a quick lunch.
She was gorgeous, as always, with her beautiful big smile and thick black hair. Red is my favorite color on her!
Her nails were beautiful, as always – a glossy, cornflower blue polish (I am sure someone knows its name). And, she happily posed for a photo.
Her very strong nails are a gift from her father. She doesn’t wear gels, just regular nail polish! I always admire those lucky people who enjoy sturdy nails. 🤗
What did we talk about? Well, lots of things:
Children
Grandchildren (new photos of her darling grandsons)
Nails
Her brain 🧠
Her corpus callosum
Everyone’s right and left brains
Scientists
My anatomy lessons and FF using Sam as model
Titans of Fantasy panel
The following is a bit of what we talked about.
I complimented her for her splendid performance at the “Titans of Fantasy” panel. Her responses were thoughtful and informative which held my attention. Made me proud!
I shared how her explaining her scientific journey to audiences delights me. Not everyone grasps what it means to be a scientist or the rigorous work entailed in becoming one. I think she helps people appreciate what science can contribute to a person’s life skills.
We talked about how science trains the left brain for details and analysis and how she patently trusts the intuitive side of her right brain.
I reminded her that the last time we met, I said she had an admirable corpus callosum because she clearly engages both sides of her brain.
Her very logical response was, “Well, why would you only want to use one side of your brain and leave the other side behind?”
To which I replied… “Pulling it along like a dog on a leash?” 😜
This may seem weird talk to you, but we always discuss things that others might find odd. (I make it a point not to press her for Outlander info. She is my friend.)
As a note of explanation, the corpus callosum is an area deep in the brain which allows right and left sides of the brain to communicate. And her sides communicate very well, indeed!
Forty-five minutes flew by and suddenly, it was time to go, she had another panel starting in minutes. This time it would be solo with no backup if she were to be late!
We headed back toward Javits, stopping at the Equinox Hotel where her ride awaited her. Her publisher was also waiting and took this photo of us, which I absolutely adore! ❤️
Then a quick hug goodbye and I returned to the Javits Center to grab a seat for the “Diana Gabaldon Spotlight’ panel.
Unfortunately, seating was very close so this was the best video I could shoot. Apologies to the lady in front!
Which part of her panel was your favorite?
I loved hearing the excerpt from book 10! ❤️
But, in addition, I enjoyed learning about her writing Outlander on her husband’s garage computer! 😮
“Who’s Jamie?” 😂😂😂
If only he knew at the time what a juggernaut her “practice book” would become!
That evening, I joined members of the FB group, Hudson Highlanders, for dinner. It was wonderful to meet these lovely ladies, two of whom I had only met via Zoom (L to R: Tonise, Lynn, Gwen, Susan)! 🤗
Then to bed for an early rise.
Next morning, I had to say goodbye to Jim and Jody. We have room-shared many times at various comic cons and they are the best!
In front of the red and white Empire State Building. I think they look like newlyweds although they have been married 36 years!
Farewell my friends, old and new. Until next time!