Hey, anatomy students! Are you interested in hernias? If yes, you came to the right place! Today’s lesson, Inguinal Hernia, is prompted by Dr. Claire performing a hernial repair in Outlander episode 408, Wilmington. Let’s pass through the stones and review the scene as it unfolds at a local 18th century theater!
Warning: Two images in this lesson show the groin area. One is of Jamie at Lallybroch millpond, the second is a clinical image. I think all readers are adults and will be OK with these. But, the warning is for those who might find such content objectionable.
After meeting Governor Tryon and his associate, Edmund Fanning, Claire observes Fanning in distress. Turns out, he suffers paroxysms of pain from a strange protrusion, incurred after standing against a mob in Hillsborough. His boots stayed in the mud as his body turned after delivering rum to appease rioters. Oh, my!

Talk about theater! Barely watching that dreadful play, Jamie learns his Godfather is in peril and devises a plan. Hum….mayhap a poke in the puir fellow’s aching belly will buy valuable time? A quick jab to the left and Fanning needs a surgeon!

Talk about belly aching! Call Surgeon Sasseynach….. STAT!

Claire to the rescue! She speedily diagnoses an inguinal hernia – confirming her earlier suspicions:
“The intestines have moved and the blood flow may be cut off!”
Fanning is quickly laid on a table as Claire marshals helpers, knife, needle, thread, linens and rum. Lots of linens and lots and lots of rum!
That is quite the lump, Edmund! A left inguinal hernia but a bit too high on the abdominal wall!

She drapes and swabs the surgical field, sterilizes a knife in alcohol and flame, threads a needle, grinds the wheat and bakes the bread! <G>

Claire begins surgery with the knife positioned near the hernia, poised to cut above the bulge and parallel to it. Good choice, Claire!

Then, inexplicably, she switches direction and cuts across the hernial bulge!!! Bad choice, Claire! 😱
She cuts very deep and there’s a lot of blood!

Then, with considerable effort, she shoves the hernia (see below) towards the midline of the body (linea alba). Pushing bowel the wrong direction, Claire!!! 😱

She skillfully sutures the wound with very what appears to be carpet thread. Not surprising, as it was likely salvaged from the costume department.

And, unlike the actors of that dreary, lugubrious play, Claire receives a standing ovation for a job well done!

Now for the science. Yay!
Hernia Defined: Simply put, a hernia is a protrusion or bulge caused by an organ or tissue pushing through the wall enclosing it (Image A).
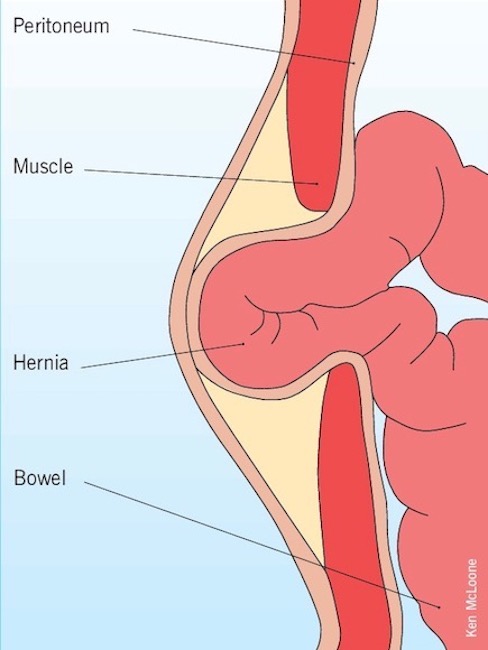
Image A
Types of Herniae: Hernae (pl) occur in different body areas, but the most common site is the abdominal wall (Image B). These include:
- epigastric (between tip of breastbone and navel)
- inguinal (groin area)
- femoral (upper thigh)
- umbilical (navel)
- incisional (surgical scar)
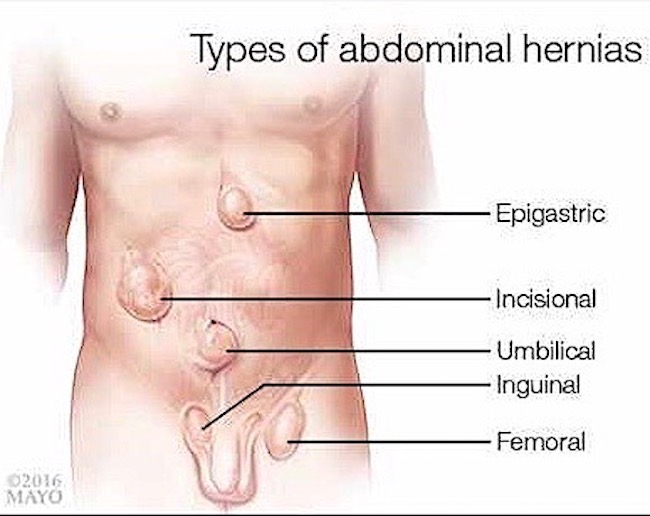
Image B
Understand that groin herniae are the most common type of abdominal herniae; these include both inguinal and femoral types. As Claire diagnosed an inguinal hernia, the lesson will cover only this type.
Inguinal Region: Inguinal herniae occur in the inguinal region. But wait! Where, exactly, is the inguinal region? Our fav anatomical model volunteers to demo! Yay, Jamie! Here, from the sky-blue waters of the freezing mill pond (Starz ep 112, Lallybroch), Jamie kindly lends a sneak-peak!
Specifically, the inguinal region is the area between anterior superior iliac spine (ASIS) and the pubic tubercle (red arrows). Can you see it? Of course, you can. Focus, students!
Both ASIS and pubic tubercle are easily palpable landmarks of pelvic bones, especially in the lean and physically fit.
The very strong inguinal ligament spans these two bony points. The ligament is overlaid by a skin crease, the inguinal groove, the site where torso meets thigh. Also, female inguinal grooves are more horizontal; male inguinal grooves are more vertical. This is because female hips are wider and the paired ASIS are further apart.
(Psst…..please forgive the blue mask overlying Jamie’s upper torso. This is to discourage bots from tagging this image as sexually explicit and landing OA in FB jail!!!)
Try This: Lay on your back and feel the prominent point of one hip bone (ilium), this is the ASIS. Now, move finger to pubic bone and feel a bump at the upper-outer margin, this is the pubic tubercle. The inguinal ligament spans these bony landmarks.

Inguinal Hernia: The inguinal hernia is a bulge in the abdominal wall above the inguinal groove. There are direct and indirect inguinal herniae. Both types are strictly defined based on their relationship to an abdominal artery and vein (inferior epigastric vessels, IEV)
- Indirect inguinal hernia produces a bulge above the inguinal ligament that is lateral to the IEV.
- Direct inguinal hernia produces a bulge above the inguinal ligament that is medial to the IEV.
Why is it important to diagnose the type? Because this may help determine how the hernia will be treated.
Image C shows right-sided indirect inguinal herniae of a male (L panel) and a female (R panel); both herniae lie above the inguinal groove and developed lateral to the IEV. This image also shows how the female inguinal groove is more horizontal than the male.
Inguinal Herniae Statistics:
- can develop at any age
- direct inguinal hernia 10x more common in men than in women
- indirect inguinal hernia 25x more common in men than in women
- more common in men above age 40
- more common on R than L side
- more common in people with a family history

Image C
Symptoms: Symptoms of an inguinal hernia include (Image D):
- bulge of inguinal region which may extend into scrotum or labia
- pain/discomfort with coughing, exercise or defecation
- pain increases during the day and lessens when lying down
- bearing down enlarges the bulge
- heartburn, chest pain, pain with eating
- redness or other discoloration of the bulge
Importantly, some inguinal herniae may be asymptomatic! Regular physical exam and complete history should consider this possibility.

Image D
Descent of Testes: There are two very important reason why inguinal herniae are more common in males than in females:
- Males tend to do more manual labor requiring heaving lifting thereby straining the abdominal wall. Usually accounts for direct herniae.
- Testes descend through the inguinal area during intrauterine life. Usually accounts for indirect herniae. Wait! What???
Yes. Ovaries and testes develop in the abdominal cavity. Over time, ovaries descend as far as the pelvis but testes continue to descend into the scrotum, a process that typically completes about week 28 of pregnancy.
Testicular descent is complicated but Image E offers a simplified visual. Descent through the inguinal region involves passing through layers of abdominal muscle and connective tissue (fascia), layers which follow the testes all the way into the scrotum. In addition, a finger of peritoneum, the membranous lining of the abdominal cavity, is dragged along with the descent. This finger of peritoneum is the processus vaginalis.
The channel created by passage through the abdominal wall is dubbed the inguinal canal. Now, this is not a canal in the usual sense, but rather a slit-like passageway. The canal also has internal (deep) and external (superficial) inguinal rings, but these are difficult to explain and not particularly useful in today’s lesson.
If all works as nature intends, each processus vaginalis closes after descent is complete. However, these may fail to close or reopen later in life, leading to an indirect inguinal hernia.
Females also develop an inguinal canal and processes vaginalis but these are smaller and usually close off more readily because no testicular descent is involved.
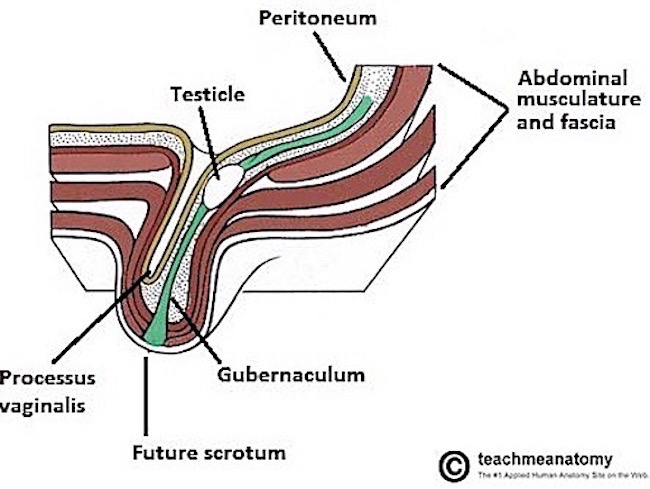
Image E
Indirect Inguinal Hernia: For your viewing pleasure, this simple cartoon illustrates testicular descent. As you view the video, notice the cream-colored “finger” that accompanies the testis into the scrotum. This finger is an extension of the peritoneum, the membrane that shrink-wraps all surfaces of the abdominal cavity and its organs.
Image E correctly labels this finger-like extension of peritoneum (tan in Image E) as the processus vaginalis. To reiterate, normally, after testicular descent, the processes vaginalis closes off.
If the processus vaginalis does not close off, or reopens later in life, then fluid, fat or loops of bowel may slither and slide down into the patent processus vaginalis forming a hernia. Not good!
Image F demos such unruly outcomes:
- Left panel shows a testis in normal position in the scrotum – no remnant of the processus vaginalis is present (patient facing to your R)
- Right panel shows a partially open processus vaginalis containing a loop of inflamed bowel.
- Middle panel shows a more extreme situation where the processus vaginalis is open all the way and bowel has slipped down into the scrotum.
If bowel becomes trapped in the processus vaginalis, its blood supply may be diminished, a condition known as incarceration or strangulation. This is a medical emergency because if the bowel dies due to insufficient blood supply, its wall breaks down allowing bacteria to seed sterile body spaces. Untreated, this leads to septicemia and death, especially in the 18th century! So, Claire is correct about surgery being necessary to save Fanning’s life.
A direct hernia works much the same way except the cause is a weaken lower abdominal wall usually from age, pregnancy, heavy lifting, etc. Here, a sac of peritoneum balloons out through the lower abdominal wall wherein bowel may become strangulated with similar fearsome outcomes. Here, intestine cannot enter the scrotum or labia because no processus vaginalis is involved.
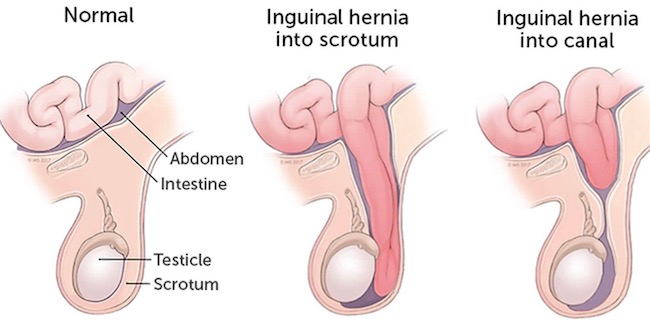
Image F
Claire’s Repair: Today, various techniques are used to repair inguinal hernias. Mr. Fanning’s hernia required pushing the bowel back into place followed by suturing the muscle and fascia layers and then the skin. No mesh in those days!
Fanning’s special FX were pretty good. However, I must make the following observations:
- Fanning’s hernia lies too high on the abdominal wall for an inguinal hernia. It should be nearer the inguinal groove or pubic bone. Perhaps the site was chosen to avoid TMI?
- No surgeon worth their salt would dare cut across a hernial bulge for risk of cutting into the bowel itself! Claire’s initial knife position was correct, why she switched position was puzzling. Perhaps, to make FX more buzz-worthy?
- Too much blood oozed from the skin cut which is also too deep – inguinal skin doesn’t bleed that much and is thin. Again, this may have been designed to produce a collective viewer’s gasp.
- The FX that really caused me to cringe is the force Claire employs to push the bowel toward the body midline! Nope. That direction, the bowel has no place to go. No wonder Fanning screams! If his is an indirect inguinal hernia, Claire should push the bowel toward his upper left (toward ASIS) following the inguinal groove. If his is a direct inguinal hernia, Claire should push the bowel directly downward so it re-enters the abdominal cavity.
- That is one honking thread Claire uses to close the wound! It will likely cause a foreign body reaction accompanied by chronic discomfort but infinitely preferable to dying from an incarcerated bowel!
- As Edmund’s bowel was incarcerated, the overlying skin should have appeared inflamed. It didn’t.
Quotes from Outlander books always enrich any anatomy lesson and this is no exception. The inguinal hernia makes its debut In Drums of Autumn book, wherein Claire repairs one on mountain man, John Quincy Myers – atop Auntie Jo’s dining room table – in front of dinner guests! Based on the description, Myers has an indirect inguinal hernia (see Image F, middle panel).
I checked that my supplies and suture needles were ready, took a deep breath, and nodded to my troops.
“Let’s go.”
Myers’s penis, embarrassed by the attention, had already retreated, peeping shyly out of the bushes…Ulysses himself delicately cupping the baggy scrotum away, the hernia was clearly revealed, a smooth swelling the size of a hen’s egg, its curve a deep purple where it pressed against the taut inguinal skin.
I swabbed the perineum thoroughly with pure alcohol, dipped my scalpel in the liquid, passed the blade back and forth through the flame of a candle by way of final sterilization, and made a swift cut.
Not large, not deep. Just enough to open the skin, and see the loop of gleaming pinkish-gray intestine bulging down through the tear in the muscle layer. Blood welled, a thin, dark line, then dribbled down staining the blanket.
I extended the incision, swished my fingers thoroughly in the disinfecting bowl, then put two fingers on the loop and pushed it gently upward.
…I could feel the movement of his intestines as he breathed, the dark wet warmth of his body surrounding my gloveless fingers in that strange one-sided intimacy that is the surgeon’s realm. I closed my eyes and let all sense of urgency, all consciousness of the watching crowd drop away.
…Time stopped. I was acutely aware of each movement, each breath, the tug and pull of the catgut sutures as I tightened the inguinal ring, but my hands did not belong to me.
…Then it was done, and time began again.
“Done,” I said, and the hum from the spectators erupted into loud applause. Still feeling intoxicated—had I caught drunkenness by osmosis from Myers?—I turned on one heel and sank into an extravagant low curtsy, facing the dinner guests.
My favorite part of Fanning’s surgery comes when the 18th century physician bustles in declaring “What hath hell wrought?” Yeah, women didn’t do surgery or openly practice medicine in those days.
Then, he accused Claire of butchering the poor man, finishing with: “All he needed was some smoke up the rear.” Bwahahaha! Priceless!

This entertaining 10 minute video by Dr. Carlo Oller does a terrific job of summarizing much of today’s lesson as well as providing additional tips about hernia prevention and care. Hope you watch!
OK, anatomy students. That is it for today’s lesson. Anatomy of the inguinal region and its associate pathology are complex, but it behooves us all to stay vigilant for signs and symptoms of a hernia.
Let’s close with this simple thought: as inguinal hernias occur more frequently in males than females, shouldn’t these be called, himnias? Wink. Wink.
A deeply grateful,
Outlander Anatomist
Photo Credits: Starz ep 112, Lallybroch, ep 408, Wilmington.
Image A www.study.com, Image B www.newsnetwork.mayoclinic.org, Image C www.laparoscopythane.com, Image D www.verywellhealth, Image E www.teachmeanatomy.info; Image F www.bodyadvances.com